Contents
1 Introduction
Every patient has the right to receive high quality care that is safe, effective and respects their privacy and dignity. Responsibility for these rights does not lie with one individual or group, but with all staff at all levels.
The NHS Operating Framework issued in 2011 to 2012 required all providers of NHS funded care to confirm whether they are compliant with the national definition “to eliminate mixed sex accommodation except where it is in the overall best interests of the patient or reflects their patient choice. This reporting requirement remains in place.
In November 2006 the Department of Health launched a ‘Dignity in Care Campaign’ with an aim to put dignity and respect at the heart of care services extended into mental health services in 2007, and is now applicable in all health and social care settings. This campaign issued the 10 point dignity challenge to organisations (appendix A).
Being with other patients of the same gender is an important component of privacy and dignity. It is a requirement that the trust provides wards or services in single sex bays and also has segregated washing and toilet facilities to allow patients’ dignity.
The NHS constitution states that service user experience is the most important measure of success. Positive service user or patient experience is important to and that patients report that they feel that their right to privacy, dignity and respect is upheld and actively promoted by staff and that they feel they matter at all times.
Delivering same sex accommodation (DSSA), the trust is required and committed to delivering same sex accommodation to enhance the privacy and dignity of service users. The trust believes that every service user has the right to receive high quality care that is safe, effective and respects their dignity and this is one of the guiding principles of the NHS constitution. There are no exceptions to delivering high standards of privacy and dignity and staff should always take the utmost care to respect this.
1.1 Definitions
1.1.1 Same sex accommodation is (DOH 2009 eliminating mixed sex accommodation)
- Same sex wards, a ward with all facilities, including dedicated toilet and washing facilities, occupied solely by either men or women, boys or girls.
- Mixed sex wards, with single bedrooms and same sex toilet and washing facilities (preferably en-suite) or mixed sex wards, with bed bays (multi-bed rooms) occupied exclusively by either men or women with access to same-sex toilet and washing facilities.
- Female only lounges, in consideration of the fact that due to their illness, the capacity of patients within the mental health and learning disability inpatient services can be impaired which increases their level of vulnerability it is essential that within these areas female only lounges are provided.
In mixed-sex wards, it is good practice to create separate parts of the ward for men and women and designated areas or zones, for the bedrooms and toilet or washing facilities for each sex. There may be times, albeit not ideal, when a corridor or the bedroom area of a ward may be mixed. If this occurs, bedrooms, toilet and bathing facilities should be designated to achieve as much gender separation as possible and care supported by appropriate staffing. Each inpatient area has in place guidance which staff are to refer to for full details as to the safe management of instances when male and female patients need to be accommodated on the same bedroom corridor (see appendices).
Men and women should not have to pass through the bedrooms or bed bays of the opposite sex to access their own bedrooms or toilet or washing facilities. Ideally, service users should not pass through mixed, communal areas adjacent to their bedrooms or bed bays to access their washing facilities. The exception is toilet facilities used while in day areas where service users are fully dressed.
Some toilets and bathrooms contain specialist facilities which are fixed (for example, hoists) to make them accessible for disabled users. Such facilities may be designated unisex as long as they are for use by one person at a time, are lockable from the inside (with external override) a risk assessment has been conducted and where necessary, the service user is escorted by a member of staff. The ideal remains to have segregated accessible facilities where this is possible.
Privacy, refers to freedom from intrusion and relates to all information and practice that is personal or sensitive in nature to an individual (DOH 2009). Privacy is a key principle, which underpins human dignity, and remains a basic human right and the reasonable expectation of every person. (Human Rights Act,1998).
The seven privacy and dignity benchmarks are:
- attitudes and behaviours
- personal world and personal identity
- personal boundaries and space
- communicating with staff and people who use our services
- privacy of service user confidentiality and information
- service user modesty
- availability of an area for privacy
Dignity, to treat someone with dignity is to treat them as being of worth, in a way that is respectful of them as valued individuals, being of equal value and worth irrespective of differences such as age, race, culture, gender, sexual orientation, social background, health or marital status, disability, religion or political conviction.
In care situations, dignity may be promoted or diminished: by the physical environment: organisational culture; by the attitudes and behaviour of the nursing team and others and by the way in which care activities are carried out. Dignity applies equally to those have capacity and to those who lack it (RCN 2008).
Respect, is positive regard shown to a person as a human being as an individual, by others, and demonstrated as courtesy, good communication, taking time and equal access.
Privacy, in terms of personal space: modesty and privacy in personal care; and confidentiality of treatment and personal information. Self esteem, self-worth, identity and a sense of oneself; promoted by all the elements of dignity but also by ‘all the little things’, a clean and respectable appearance, pleasant environments and by choice and being listened to.
Autonomy, including freedom of act and freedom to decide on opportunities to participate, and clear comprehensive information.
Modesty, refers to treatment being given in a manner which avoids unnecessary exposure and minimises anxiety and distress.
2 Purpose
This policy is designed to provide:
- direction to staff to enable them to provide care and treatment to all patients, service users and carers receiving services from the trust in a way which treats them with respect and maintains their right to privacy and dignity
- a clear definition to all staff as to what constitutes privacy and dignity within a care setting
- a clear definition to all in-patient staff of same sex accommodation
- in-patient staff across the trust with guidance on the safe management of same sex accommodation
- details of the procedure for reporting any breaches in the trust compliance in relation to eliminating mixed sex accommodation
3 Scope
This policy applies to all healthcare professionals and volunteers whether directly employed by the trust, or covered by a letter of authority or honorary contract, undertaking duties on behalf of the trust working within bed based services.
4 Responsibilities, accountabilities and duties
4.1 Board of directors
The board of directors are accountable for the trust having policies and procedures in place which meet national and local requirements and, or legislation in order to provide a service which is based on best practice. The lead director responsible for this policy is the chief operating officer.
4.2 Deputy and associate nurse directors for inpatient services
Deputy and associate nurse directors for inpatient services are responsible for:
- monitoring compliance with this policy
- reporting any non-compliance of this policy via the trust incident reporting system
- investigating any reported none compliance with this policy
- the implementation of any action plans arising from audits of the policy and patient feedback
- identifying training needs of staff that fall within the remit of this policy
4.3 Matrons or managers
Matrons or managers are responsible for:
- making staff aware of this policy, it’s content and where to access the policy
- reporting any non-compliance of this policy, or concerns about any poor practice by staff to the associate nurse director
- assisting in the investigation of any failure to comply with the policy including all breaches and taking corrective action to prevent any reoccurrence
4.4 Healthcare professionals
All healthcare professionals must:
- actively promote the patients privacy and dignity at all times
- ensure that all service users are cared for in single sex accommodation as defined by this policy
- be aware of their role if acting as a chaperone
- report any breaches of the policy or EMSA to their line manager and on the trust’s incident reporting system (IR1)
5 Procedure or implementation
5.1 Breaches of policy (CQC supporting note mixed sex accommodation)
A breach occurs at the point a patient is admitted to mixed sex accommodation outside the terms of this policy or if there isn’t a ladies only lounge in a mental health or leaning disability facility.
Mixing may be justified (for example, not a breach) if it is in the overall best interest of the patient, or reflects their personal choice.
5.1.1 Reporting of breaches
All potential breaches of sleeping accommodation must be reported for each patient affected via the trust Incident reporting system IR1.
5.1.2 Acceptable justification physical health (not a breach only)
- In the event of a life threatening emergency either on admission or due to sudden deterioration in a patient’s condition.
- Where a critically ill patient requires constant one-to-one nursing.
- Where a nurse must be physically present in the room or bay at all times.
- Where a short period of close patient observation is needed, for example, where there is a high risk of adverse drug reaction.
- On the joint admission of couples or family groups.
5.1.3 Unacceptable justification (a breach)
- Placing a patient in mixed-sex accommodation for the convenience of medical, nursing or other staff, or from a desire to group patients within a clinical speciality.
- Placing a patient in mixed-sex accommodation because of a shortage of staff or poor skill mix.
- Because of restrictions imposed by old estate (for example, old buildings and facilities are not considered an excuse for non-compliance).
- Placing a patient in mixed-sex accommodation because of a shortage of beds.
- Placing a patient in mixed-sex accommodation because of a fluctuation in activity or seasonal pressures.
- Placing a patient in mixed-sex accommodation because of a predictable non-clinical incident, for example, ward closure.
- Placing or leaving a patient in mixed sex accommodation whilst waiting for assessment, treatment or a clinical decision.
- Placing a patient in mixed sex accommodation for regular but not constant observation.
It is not acceptable to mix sexes purely on the basis of clinical specialism. For instance in a stroke unit it may be acceptable to mix patients immediately following admission (life threatening emergency, and in need of 1-to-1 nursing) but not to maintain mixing throughout their rehabilitation phase, simply on the basis that it is easier for staff, or because there are not enough staff with the necessary skills.
5.1.4 Patient choice
There are some instances when sharing accommodation with the opposite gender reflects personal choice and may therefore be justified. In all cases, privacy and dignity should be assured. Group decisions should be reconsidered for each new admission to the group as consent cannot be presumed and in such circumstances consideration needs to be given to the patient’s capacity to make such a choice.
There are certain situations where it is in the patient’s best interest to receive rapid or specialist treatment, and same, sex accommodation is not the immediate priority. In these cases privacy and dignity must be protected. The patient should be provided with same, sex accommodation immediately the acceptable justification ceases to apply.
5.1.5 Acceptable justification (not a breach)
- If an entire patient group has expressed an active preference for sharing and all patients have the capacity to express their preference.
- If individual patients have specifically asked to share and other patients are not adversely affected (for example, children or young people who have expressed an active preference for sharing with people of their own age group, rather than gender.
5.1.6 Unacceptable justification (a breach)
- “Take it or leave it”, for example, if the patient is asked to choose between accepting mixed-sex accommodation, or going elsewhere.
- “No win situation” the patient is asked to prioritise same-sex accommodation over another aspect of their care, for example, speed of admission, specialist staff etc.
- Custom and practice, for example, routine mixing of young people without establishing preferences.
- If the patient said they did not mind (there should always be a presumption of segregation unless patients specifically ask to share).
- If the patient did not express a preference.
It is important to note that it is always the priority to aim for segregation, the circumstances in which patients choose to share are expected to be in the minority.
5.1.7 Exceptional circumstances
There will be specific circumstances where mixing is acceptable as an emergency to extreme operational emergencies. This is limited to unpredictable events such as major clinical incidents, for example, a multiple road traffic accident or natural disaster and major non clinical incidents such as fire, or flood requiring immediate evacuation of buildings.
5.1.8 Maintaining same sex accommodation in the event of an outbreak
The trust’s major incident PlanT’ critical and major incident plan sets out a framework for organisational responses to any kind of major incident affecting service users and, or staff. This alongside the business continuity policy for each of the trust’s individual services or departments will support the ongoing provision of same sex accommodation during any such outbreak.
5.2 Special considerations
5.2.1 Single sex wards
Within the trust there are a number of single sex wards but this policy still applies to these in relation to the maintenance of patient’s privacy and dignity, and the right of the patients to be treated with respect.
5.2.2 Transgender or transsexual service users
‘Trans’ is an umbrella term that represents those who are transsexual or transgender but it also refers to those who are transvestite or any other form of gender fluidity. Many who are transgender prefer to use the term ‘trans’ out of choice and it has been adopted by many individuals in the UK.
As part of the ‘transitioning’ or gender reassignment process people have to live in the gender with which they identify, which means they will change their name and personal details. They may or may not seek treatment such as cross-sex hormones and surgery. A birth assigned male who transitions to a female gender role is a trans-woman. Similarly, a birth assigned female who transitions to a male gender role is referred to as a trans-man.
It is not appropriate to refer to someone’s trans status, unless they refer to it first, and until then they should be simply referred to by their name or as she or he, female or male or women and men. If you call someone by the wrong gender (misgender), after you have been informed by the patient, you are potentially committing a hate crime, which could be a criminal offence under the Criminal Justice Act 2003 and is against the Human Rights Act 1998.
Once a trans person formally changes their name and gender role, all NHS records should be amended to reflect this change. A gender recognition certificate (GRC) is not necessary for this to be effected. The patient’s trans identity should not be disclosed to staff outside of the treating team and should only be shared on a “need to know basis” within teams. Section 22 of the Gender Recognition Act 2004 makes it a criminal offence to disclose a person’s trans identity to somebody else if obtained in an official capacity and without their express permission.
A significant number of trans individuals experience difficulties when accessing healthcare (Whittle et al., 2007). This may be due to prejudice and, or lack of knowledge by healthcare staff.
Trans individuals may present to mental health services at any stage of their transition or treatment; or, after treatment has finished. This may be due to distress relating to gender dysphoria or to discrimination and victimisation (minority stress) as well as, issues unrelated to their trans status.
Trans individuals have a higher rate of self-harm behaviour and suicide than the general population (Whittle et al 2007; Dhejne et al., 2011; Claes et al., 2014). Public Health England has data that states 90% of the trans community have thought about or attempted suicide. With this in mind, mental ill-health amongst this population will be significantly higher. It is important to note that like anyone else trans individuals may experience psychiatric morbidity, unrelated to any gender issues, which may need medical treatment, counselling or psychotherapy.
As with any individual where health issues, both physical and, or mental, have become such a problem as to reach the threshold for entry to secondary care, trans individuals should be able to access services as any other patients.
The Department of Health guidance on the treatment of trans people in the NHS (2008) gives little specific guidance for in-patient accommodation. There are, however general principles which should be applied:
- staff should be alert to the possibility of any of their patients having issues relating to their gender
- these need to be approached sensitively
- should there be any doubt regarding the patient’s gender identity, the patient should be asked how they wish to be addressed
Key guidance states, Trans people should be accommodated according to their presentation:
- the way they dress
- the name and pronouns that they currently use
- this may not always concur with the physical sex appearance of the chest or genitalia
- it does not depend upon their having a gender recognition certificate (GRC) or legal name change
- it applies to toilet and bathing facilities (except, for instance, that preoperative trans people should not share open shower facilities)
- views of family members may not accord with the trans person’s wishes, in which case, the trans person’s view takes priority
5.2.2.1 In detail
- If the patient is transitioning or has completed their transition then they should be referred to by the name and pronouns they identify with and the patient’s wishes adhered to.
- The patient should be accommodated in a gender neutral environment such as a side-ward.
- The patients should be treated with sensitivity, dignity and respect and protected from abuse by other patients or visitors.
- Patients who are transitioning irrespective of evidence of name change or whether they have completed treatment, should always be treated as the gender of their identity.
- It would be grossly inappropriate to nurse such a patient on a single-sexed ward of their birth gender.
- It may be appropriate to discuss with the patient how they wish to be nursed and any special requirements they may have.
- Trans individuals should not be treated less favourably than other people when being looked after in hospital.
Patients who are detained in psychiatric hospitals, including secure facilities, may present with particular difficulties. A detained patient may have difficulty making a social gender role change and it is unlikely that such a patient would be able to judge from hospital as to whether it is possible for them to live in another gender in the community. However, there may be some patients for whom living in the community may never be feasible or not for some years and therefore appropriate accommodation needs to be made.
5.2.2.2 Equality Act 2010
Protects individuals from unfair treatment and promotes a fair and equal society. It places a statutory duty on all public authorities to eliminate unlawful discrimination and harassment and promote equality of opportunity between men and women including transmen and trans-women.
Section 7 states:
- “a person has the protected characteristic of gender reassignment if the person is proposing to undergo, is undergoing or has undergone a process (or part of a process) for the purpose of reassigning the person’s sex by changing physiological or other attributes of sex”
In order to meet the needs of these service users in a non-discriminatory way staff will ensure that:
- where possible transgender patients are accommodated according to their presentation (the way they dress, and the name and pronouns that they currently use). This presentation may not always accord with the physical sex appearance of the chest or genitalia and does not depend on them having a gender recognition certificate (GRC) or legal name change
- if due to an identified risk to their personal safety or wellbeing they cannot be safely accommodated according to their presentation a full explanation is given as to the reasons why and what measure are to be put in place to support them during their inpatient stay
- all transgender patients are cared for in a single room
- transgender patients do not share open shower facilities
- the views of the transgender patients take precedence over those of family members where these are not the same
5.2.3 Electro convulsive therapy
Within RDaSH there is1 ECT department based at the Woodlands older peoples mental health unit at Oakwood Hall Drive, Rotherham. Please see electro-convulsive therapy (ECT) clinical guidelines policy for further information.
6 Training implications
There are no specific training requirements in relation to this policy, but all trust staff will need to be familiar with this document.
As a trust policy, all staff need to be aware of the key points that the policy covers Staff will be made aware of its content via any of the following:
- team brief
- daily email system
- team meetings
- supervision
- practice development days
- induction
7 Monitoring arrangements
7.1 Any none compliance with the policy
- How: Investigation of any formal, informal complaints or your opinion counts forms which relate to none compliance with the contents of this policy. Investigation of any IR1 reports which relate to breaches of EMSA. Monitoring any none compliance reported on the IR1 electronic reporting system.
- Who by: Modern matrons or managers deputy director of nursing.
- Reported to: Business divisions leadership and quality groups trust performance report.
- Frequency: Ongoing. By exception.
8 Equality impact assessment screening
To download the equality impact assessment for this policy, please follow this link: EMSA policy EIA.
8.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, ‘not just clinically but in terms of dignity and respect’.
As a consequence the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
8.1.1 How this will be met
The content of this policy emphasises the need throughout that the service user’s privacy and dignity are respected.
8.2 Mental Capacity Act
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals capacity to participate in the decision making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
8.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005).
9 Links to any other associated documents
- MCA Mental Capacity Act 2005 policy
- Electro-convulsive therapy (ECT) clinical guidelines policy
- Consent to care and treatment policy
- Interpreters policy (provision, access and use of, for patients, service users and carers)
- Safeguarding adults policy
- Critical and major incident plan
10 References
- Dept of Health (2001, 2010) Essence of Care Benchmarks DH, London.
- Dept of Health (2006) Dignity in Care Challenge DH, London.
- Dept of Health (2007) Privacy and Dignity, A Report by the Chief Nursing Officer into mixed sex accommodation in hospitals. DH, London.
- Dept of Health (2009) Eliminating Mixed Sex Accommodation DH London.
- Dept of Health (2010) Eliminating Mixed Sex Accommodation PL/CNO/2010/3 DH London.
- Dept of Health (2011) Eliminating Mixed-Sex Accommodation, Declaration Exercise Gateway Reference 15552 DH London.
- RCN (2008) Definition of Dignity Publication code 003 298.
- Mental Health Act, Code of Practice (2015).
- Department of Health (2010) Dear Colleague letter from the Chief Nursing Officer and Deputy NHS Chief Executive. Eliminating Mixed Sex Accommodation, November 2010.
11 Appendices
11.1 Appendix A The 10 point dignity challenge
High quality services that respect people’s dignity should:
- have a zero tolerance of all forms of abuse
- support people with the same respect you would want for yourself or a member of your family
- treat each person as an individual by offering a personalised service
- enable people to maintain the maximum possible level of independence, choice and control
- listen and support people to express their needs and wants
- respect peoples’ right to privacy
- ensure people feel able to complain without fear of retribution
- engage with family members and carers as care partners
- assist people to maintain confidence and a positive self-esteem
- act to alleviate people’s loneliness and isolation
11.2 Appendix B Bed management and delivering single sex accommodation on the adult acute mental health wards
Whilst the adult acute mental health wards are not single sex they are designed to provide single ensuite bedrooms on corridors which are designated as single sex. However due to demand for inpatient beds there may be times when the ratio of male and female patients is not balanced to the available beds and in these circumstances staff should take the following action:
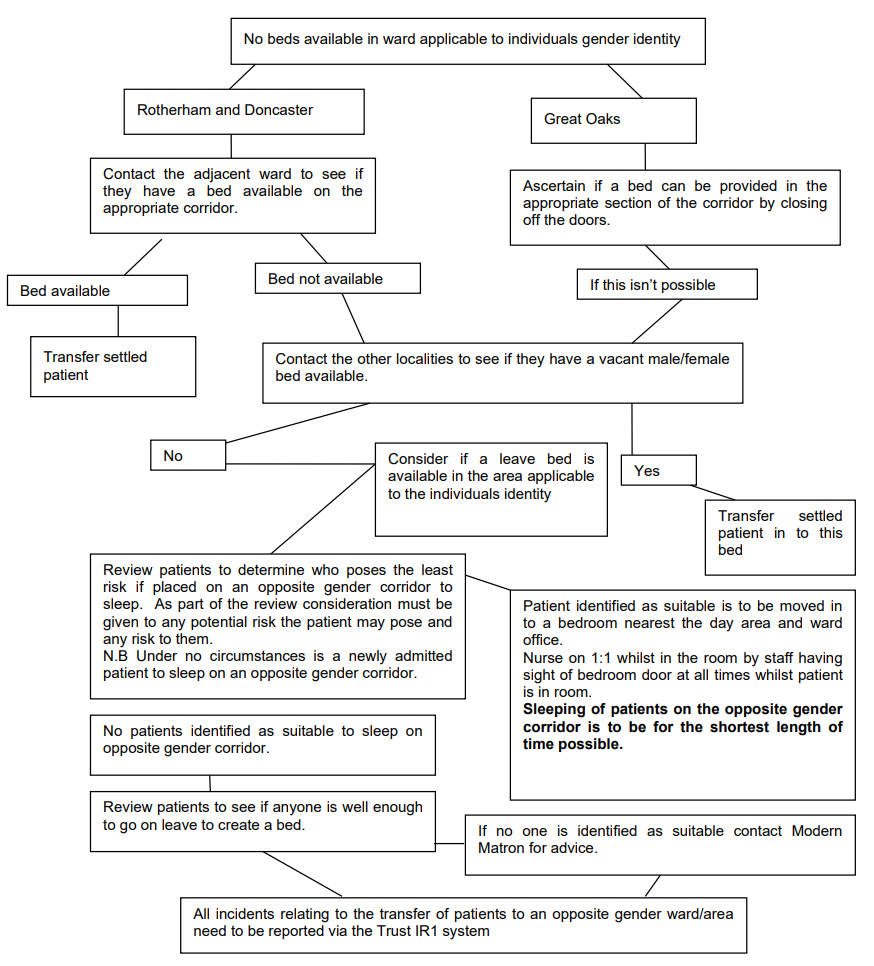
- No beds available in ward applicable to individuals gender identity.
11.2.1 Rotherham and Doncaster
- Contact the adjacent ward to see if they have a bed available on the appropriate corridor.
- Bed available, transfer settled patient. End process.
- Bed not available, go to 11.2.3.
11.2.2 Great Oaks
- Ascertain if a bed can be provided in the appropriate section of the corridor by closing off the doors.
- If this isn’t possible, go to 11.2.3.
11.2.3 No beds available
- Contact the other localities to see if they have a vacant male or female bed available.
- Yes, transfer settled patient in to this bed. End process.
- No, consider if a leave bed is available in the area applicable to the individuals identity.
- Review patients to determine who poses the least risk if placed on an opposite gender corridor to sleep. As part of the review consideration must be given to any potential risk the patient may pose and any risk to them. Note, under no circumstances is a newly admitted patient to sleep on an opposite gender corridor.
- patient identified as suitable is to be moved in to a bedroom nearest the day area and ward office. Nurse on 1-to-1 whilst in the room by staff having sight of bedroom door at all times whilst patient is in room. Sleeping of patients on the opposite gender corridor is to be for the shortest length of time possible
- No patients identified as suitable to sleep on opposite gender corridor.
- Review patients to see if anyone is well enough to go on leave to create a bed.
- If no one is identified as suitable contact modern matron for advice.
- All incidents relating to the transfer of patients to an opposite gender ward or area need to be reported via the trust IR1 system. End process.
11.3 Appendix C Bed management and delivering single sex accommodation on Laurel ward (older person’s mental health, North Lincolnshire)
Whilst Laurel ward is not single sex; it is designed to provide single en-suite bedrooms within zones in corridors which are designated as single sex. However due to demand for inpatient beds there may be times when the ratio of male and female patients is not balanced to the available beds and in these circumstances staff should take the following action:
- If a vacant bed is not available in the appropriate gender zone a leave bed in the appropriate zone is to be used if it is available.
- If no leave bed is available undertake a risk assessment of the patient being admitted.
- Consider moving existing patients within the 4 zones so that each zone is single sex, ensuring that low risk patients of opposite sex are in the rooms at the zone boundaries.
- Where male patients are assessed as low risk but require being in a female zone either because all zones have females in or the patient needs a specific room, for example, bariatric or disabled bedroom; then both the risk assessment and the rationale for the decision must be clearly documented in the patient record.
- If the patient is unknown or the patient is assessed as potentially posing a risk to females the patient must be nursed on a 1-to-1 whilst in the room by staff having sight of bedroom door at all times whilst patient is in room. Sleeping of patients with risks in an opposite gender zone is to be for the shortest length of time possible.
- Any decision to place a male patient in a zone of the opposite sex must be discussed with the modern. Authority to use additional staff can be sought from matron or manager in hours or the on call manager out of hours if required to minimise risk.
- All incidents relating to the transfer of patients to an opposite gender ward or area need to be reported via the trust IR1 system. End process.
11.4 Appendix D Bed management and delivery of single sex accommodation at Sapphire Lodge, Doncaster
Both units, Sapphire Lodge and Rhymers court are equipped with single bedrooms with ensuite shower rooms.
At Sapphire Lodge we have two wings and wherever possible operate these as male and female wings to promote privacy and dignity. Should there be an imbalance of gender, then all patients are reviewed and risk assessed to identify the safest and most sensible way forward to offer both privacy and dignity to both genders if sharing a wing.
Rhymers court has individual living areas, bungalows which again operate a similar process to Sapphire Lodge. Wherever possible the bungalow would be single gender, or take the similar approach to provide a safe mix of genders within a bungalow, whilst still offering single en-suite bedrooms. As with the adult mental health wards, if mixing genders is required due to circumstances, the pathway on the following page would be followed.
All incidents relating to the transfer of patients to an opposite gender ward or area need to be reported via the trust IR1 system.
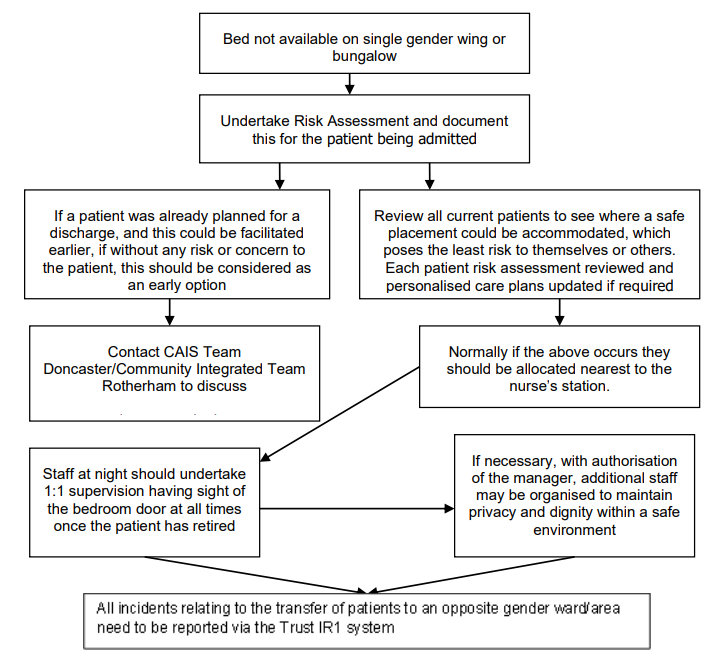
- Bed not available on single gender wing or bungalow.
- Undertake Risk Assessment and document this for the patient being admitted.
- if a patient was already planned for a discharge, and this could be facilitated earlier, if without any risk or concern to the patient, this should be considered as an early option
- contact CAIS Team Doncaster or Community Integrated team Rotherham to discuss. End process.
- Review all current patients to see where a safe placement could be accommodated, which poses the least risk to themselves or others. Each patient risk assessment reviewed and personalised care plans updated if required.
- Normally if the above occurs they should be allocated nearest to the nurse’s station.
- Staff at night should undertake 1-to-1 supervision having sight of the bedroom door at all times once the patient has retired.
- If necessary, with authorisation of the manager, additional staff may be organised to maintain privacy and dignity within a safe environment.
- All incidents relating to the transfer of patients to an opposite gender ward or area need to be reported via the trust IR1 system. End process.
11.5 Appendix E Bed management and delivery of single sex accommodation on Hazel, Hawthorn and Magnolia
Hazel, Hawthorn and Magnolia are mixed sex wards with single sex bays and single rooms. When selecting appropriate placement staff need to consider dignity of new patient and others. Document decision making process in care plan.
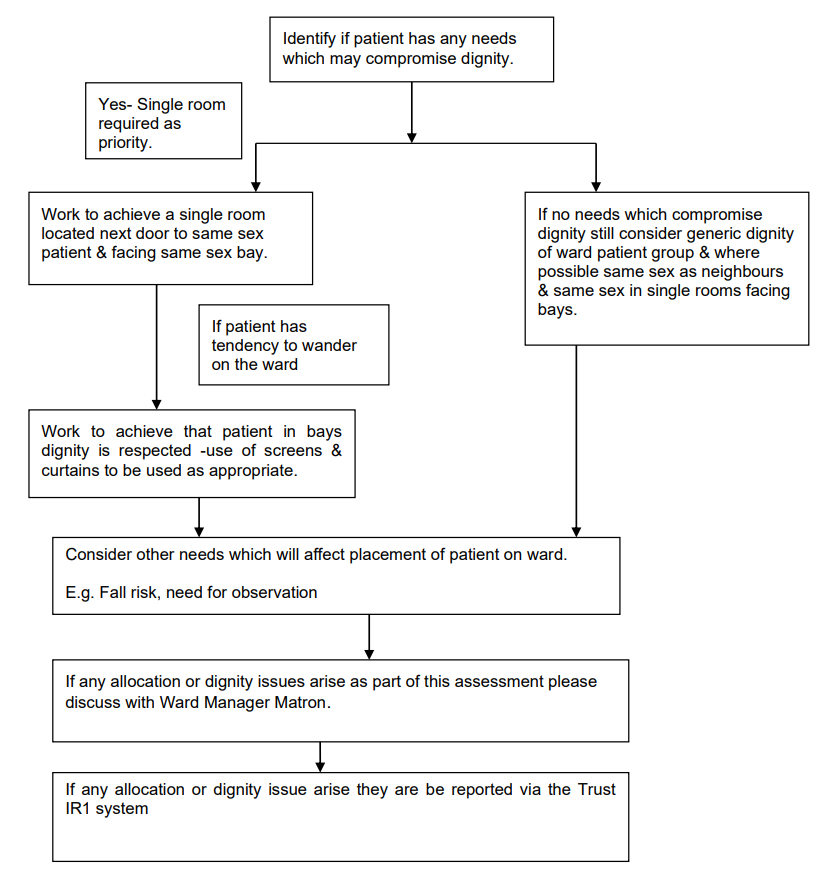
- Identify if patient has any needs which may compromise dignity.
- If no needs which compromise dignity still consider generic dignity of ward patient group and where possible same sex as neighbours and same sex in single rooms facing bays.
- consider other needs which will affect placement of patient on ward. For example, fall risk, need for observation
- if any allocation or dignity issues arise as part of this assessment please discuss with ward manager matron
- if any allocation or dignity issue arise they are be reported via the trust IR1 system. End process.
- Yes, single room required as priority.
- Work to achieve a single room located next door to same sex patient and facing same sex bay.
- If patient has tendency to wander on the ward:
- work to achieve that patient in bays dignity is respected use of screens and curtains to be used as appropriate
- consider other needs which will affect placement of patient on ward. For example, fall risk, need for observation
- if any allocation or dignity issues arise as part of this assessment please discuss with ward manager matron
- if any allocation or dignity issue arise they are be reported via the trust IR1 system. End process.
11.6 Appendix F Bed management and delivery of single sex accommodation at St. John’s Hospice in-patient unit
St. John’s Hospice inpatient unit is a mixed sex ward with ten single rooms all with en-suite facilities including a toilet and shower. When selecting appropriate placement of patients, staff need to consider the dignity of new patient and others. Staff should document their decision making process in the patients care plan.
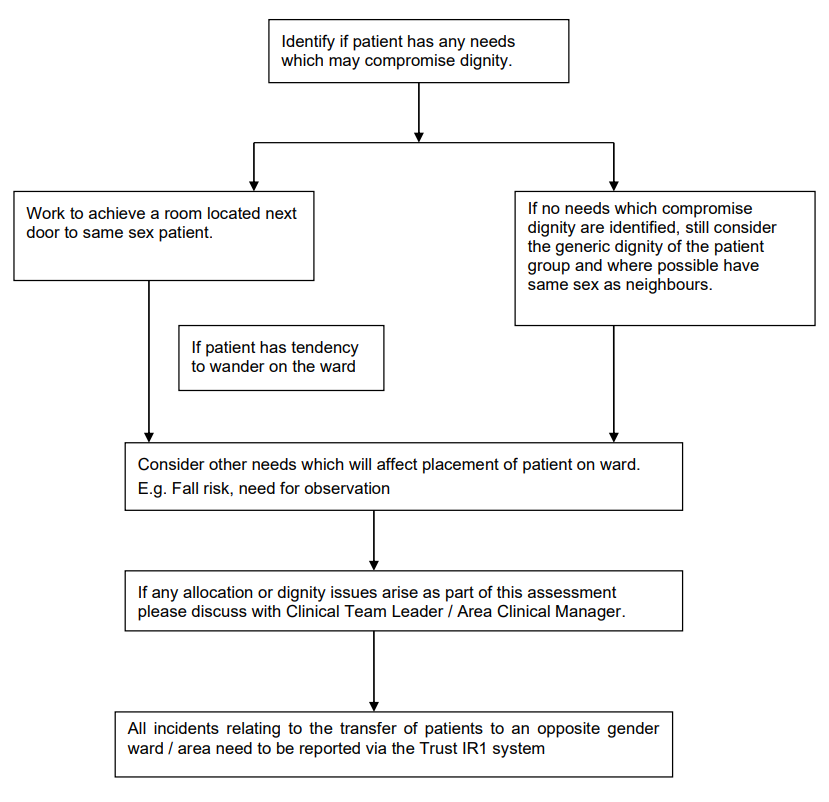
- Identify if patient has any needs which may compromise dignity.
- if no needs which compromise dignity still consider generic dignity of ward patient group and where possible same sex as neighbours and same sex in single rooms facing bays
- consider other needs which will affect placement of patient on ward. For example, fall risk, need for observation
- if any allocation or dignity issues arise as part of this assessment please discuss with ward manager matron
- if any allocation or dignity issue arise they are be reported via the trust IR1 system. End process.
- Yes, work to achieve a room located next door to same sex patient.
- If patient has tendency to wander on the ward:
- consider other needs which will affect placement of patient on ward. For example, fall risk, need for observation
- if any allocation or dignity issues arise as part of this assessment please discuss with ward manager matron
- if any allocation or dignity issue arise they are be reported via the trust IR1 system. End process.
Document control
- Version: 4.1.
- Unique reference number: 339.
- Approved by: Clinical policies review and approval group.
- Date approved: 5 November 2019.
- Name of originator or author: Nurse consultant safeguarding.
- Name of responsible individual: Clinical policies review and approval group.
- Date issued: 7 February 2020 (minor amendment, spelling).
- Review date: November 2022.
- Target audience: All staff working on in patient areas.
Page last reviewed: April 05, 2024
Next review due: April 05, 2025