For a printed or translated copy of our promises report, please contact our Communications team at:
- Phone: 03000 212 100
- Email: rdash.rdashcommunications@nhs.net
This is our second annual report on the trust’s work, with partners, to deliver the promises which form our clinical and organisational strategy 2023 to 2028 to nurture the power in our communities. This report is trust produced but it contains peer-led feedback on our work over the past twelve months, including from those members of our local communities who have been contributing within our decision-making leadership groups: part of promise 5. The report outlines the success measures for all of our promises, provides an easy read summary of the strategy, and offers an honest assessment of work done two years into five years of the hard work carried out to improve care.
Introduction
This is the second year in which we have reported back formally and very publicly on the delivery of the trust’s 28 promises: the key commitments within our organisational and clinical strategy, which we began in 2023, and intend to complete in 2028. Thank you for reading it and telling us what you think.
This year we publish both our own trust’s assessment and the feedback from our patient engagement partner organisation: the People Focused Group (PFG). They have chosen to focus their comments on the promises associated with our first objective: nurture partnerships with patients and citizens to support good health. Both points of view are important, because our strategy is about building trust within local communities. The promises are a way of nurturing the power in our communities and our partnership with patients, carers and communities is essential to our mission.
In the summer of 2025, we take another important step in that process of co-production and inclusion with the launch of our “shadow” clinical leadership executive. Bringing together patient and third sector voices, this key committee helps to set our organisational agenda and will complement the involvement of patients in all of our individual decision-making processes and the expansion of our council of governors, both achieved during 2024. A patient representative sits within our clinical leadership executive every month and the shadow group will provide wider and more diverse feedback in support of that leadership.
Over the coming nine months we expect to celebrate delivery in full of two of our promises. We aim to be accredited as a Real Living Wage employer (promise 25) this summer and by autumn to have met the measures we set for our volunteering promise 3. As the assessment in this report illustrates, we have made huge progress too with promises 4 on patient feedback and 5 on community involvement.
Care Opinion has made a transformational difference to the visibility and scale of patients’ voices within the trust. We continue to work hard to use a range of techniques to hear from those who do not want to use this technology. Taken together, these main and then complimentary approaches, are ensuring that our management systems benefit from the advice of, and weight given by, patients. This feedback sits alongside more traditional data about quality and performance.

When we report in 2026, we know that delivering our waiting time promise 14, and success in localising care through ending out-of-area placements, will be crucial steps for local people. At the same time, we need to sustain educational excellence and develop our research practice further. Promise 26 is about becoming an anti-racist organisation that fights discrimination in all forms, our work this year to largely eliminate the gender pay gap testifies to that work, which continues with successful work to deliver the board’s seven-point anti-racism plan in practice, making a meaningful difference for our staff colleagues and for the wider community.
Since February 2025, the executive leadership of the trust has focused time and effort on promises within our fourth strategic objective (18, 19, 20, 21, 22, 23): intended to create a high-quality therapeutic care model for anyone in bed-based care. That work has seen us open new facilities, and continue to transfer investment into community services both in assertive outreach in Doncaster and Rotherham and specialist community rehabilitation in North Lincolnshire.
We do not only report on these promises once a year. Every meeting of the board of directors since September 2024 has considered our progress with every measure, and from June 2025 the same scorecard has been used within the clinical leadership executive. It is really important that our assessments are open and visible, including so that they can be challenged. Doing justice to the work of so many trust colleagues, and that of partners, does not mean that we should obscure where we are behind or face real difficulties. Our commitment to environmental sustainability will need external funding to move us away from gas energy; and we cannot deliver on neighbourhood health without the deep collaboration that will be at the heart of the NHS Ten Year Plan.
The year under review has seen the trust’s groups and directorates embrace the promises we made to local partners and local people. We have extended work on our virtual ward model (promise 20) and taken major steps to align our registers of care with those of local general practice (promise 7 and 21). Alongside re-accreditation for our work with veterans (promise 11), expansion of apprenticeships (promise 9), and introduction of new clinical steps for young children before they start school (promise 17) we are starting to see the influence of the strategy on day-to-day clinical practice at the trust.
No promise is beyond our reach by 2028. By 2026 we expect to have achieved almost half our aims. At a time of huge change in the NHS, and public services, we remain fully focused on these promises, learning from our work to understand and tackle poverty (promise 6) which lies at the root of so many health challenges locally.
Kath Lavery, Chair.
Jo Cox, Lead Governor.
Toby Lewis, Chief Executive.
A reminder about the origin of our promises
These promises did not come from the trust’s board, nor from senior leaders acting alone. The trust began to consult on its strategy in 2022 with large-scale engagement among professionals inside the organisation, and with patients and partners across our communities. The final drafts of the promises were carefully considered by our clinical leadership executive before being put to the board of directors. The council of governors, as well as clinical advisory groups, also contributed to the final draft, which was approved in July 2023 and launched in September at our first leaders’ conference.
There are 28 promises because we wanted to remember that we only have until 2028 to deliver our mission. But also, that we do have until 2028: five years is time to experiment, to recognise the collaborations we need to succeed, to learn from one another. Our promises span our services for children and young people, deliberately reiterate our commitment to improving learning disabilities’ care locally, focus attention on to our equally well endeavour to create parity between mental and physical health, and acknowledge the need to change our culture as well as to create better outcomes from the services we offer. Everyone who volunteers, studies or works in the trust can find a promise relevant to their service and their values.
Clinically led, system enabled, community powered
Alongside our constant values, we want to develop the trust as a culture where power is recognised in our communities and shared better in the future than in the past. Our clinicians have to be able to lead these changes, enabled by backbone systems of administration, information, and equipment which are reliable and effective.
During 2024 and 2025, we have focused on making sure that clinical teams are fully staffed. We have fewer vacancies than ever before at the trust. Since autumn 2024, our induction of new employees has changed completely, it takes place in community venues, across a full week, and is rooted in the promises and the strategy. At the same time, our investment in leaders and leadership development programme is undertaken alongside community leaders, and with a focus on allyship, equity and power.
Reforms to core clinical pathways, included the introduction of DIALOG+ to replace the care programme approach (CPA) in mental health services, reflect the same intention as the wider mission and strategy. By focusing on a patient’s whole self and working with them to understand the outcomes important to them, we not only intend to deliver on promise 16, but to reshape models

Nothing done alone: thank you to our partners
All of the objectives and promises in our strategy depend on collaboration. These may be commercial partnerships to develop better research or to promote flexible and “bank” working. Or investments of time and money in working within the local voluntary and third sector to support peer support, specialist services for marginalised citizens, or new ways to reach into rural communities across our places. Working with teachers on glasses-for-classes, with police officers on community safety, alongside housing associations to deliver better tenancies, or with hospital colleagues to improve care for people with learning disabilities or eating disorders.
It is apparent from our promises, and from the focus of the board on primary care, that collaboration with general practice is perhaps the essential step for success. As GP leaders join the trust’s medical leadership this year, and as we work successfully to deliver health interventions to housebound patients, and to offer care in community venues like libraries and leisure centres, we want to entwine our work with that of general practice. In 2024 at our annual members’ meeting, we heard from patient voices that too many times referrals into services did not “meet a threshold” and that there is concern that services remain elusive. As we push fast and hard to make neighbourhood health meaningful in North Lincolnshire and South Yorkshire, that perception, grounded in too many realities, must change. We have commissioned Primary Care Doncaster to review the referral processes we have in place and to help us to reorganise them to better support access and to ensure continuity of care.
The trust has worked to move monies into preventive care over the past year. We have invested in what might be traditionally considered public health initiatives. The board’s public health, Patient Involvement and Partnerships Committee has worked to oversee the development of a community involvement framework, and to assess extant health and wellbeing strategies. The trust is an active member of all relevant local statutory boards, and “making every contact count” is part of our promises to local patients.
As an NHS trust we also benefit from hosting a community-interest-company (CiC), Flourish, and from our charitable trust work, Your Hearts and Minds. Both publish their own reports this summer. Through the vocational employment and social care partnerships we have with Flourish, and through the relationships developed by our community grants programme within our charity, the trust is able to innovate at pace and test ideas which are not traditional for the health service.
Looking forward, our health inequalities “radicals fund” will create an incredible opportunity to make a difference, perhaps especially in responding to promise 6 on poverty, promise 10 on inclusion health, and in delivering our “RDaSH 5” commitments under promise 8. The challenge posed by Professor Bola Owolabi, then NHS England Director for Health Inequalities, at our 2024 leaders’ conference, to deliver on Serious Mental Illness health checks for global majority patients, or the need to ensure dementia diagnosis or specialist perinatal mental healthcare is equitably available, is a crucial part of our plans for the next two years.
Radical candour
Our report seeks to meet this commitment. Healthcare can do harm. At our best, our teams and partners do incredible work. So, with our promises, there will be examples of missing the meaning or indeed not delivering the standard we aspired to. We hoped to end out-of-area placements in 2024. We did not. But in the year ahead, we will make huge progress in doing so, both by improving ward-based care and by opening new services like our North Lincolnshire Community Rehabilitation team, our trust-wide high dependency unit, and our housing association programmes like Burns Court.
Many people have shared with us the impact of poverty on their lives, and the ways in which health services do not acknowledge or respond to those realities. Thirty-three services have now completed poverty proofing reports: they are a core objective of our council of governors. The trust will play its part through ensuring access to rights and benefits, starting with addressing transport costs and digital exclusion.
Working in neighbourhoods: NHS Ten Year Plan (2025)
The trust’s strategy and promises date from 2023. With publication of the plan for the NHS, issued by the Department of Health and Social Care, in 2025, the commitments in our strategy seem “ahead of their time”. The determination to provide care in communities, through neighbourhoods, is threaded through the promises, along with a determination to work with primary care and with local voluntary sector groups.
But neighbourhood working is not new in public services. Across South Yorkshire and North Lincolnshire, there are examples of successful hyper-local collaboration. The challenge of the future is to make that more commonplace without losing the localism that is an essential part of its importance and effectiveness. Neighbourhood health is about far more than the NHS. And shaping support, care and investment around neighbourhoods must be rooted in the voices of patients and carers.
Looking forward, promise 5 in the strategy remains essential: “From 2024, systematically, involve our communities at every level of decision-making in our trust throughout the year, extending our membership offer, and delivering the annual priorities set by our staff and public governors”.
That principle of co-production and ongoing (not episodic) involvement in decision-making will be at the heart of any neighbourhood working in which the trust is a part.

Our 28 promises
- Employ peer support workers at the heart of every service that we offer by 2027.
- Support unpaid carers in our communities and among our staff, developing the resilience of neighbourhoods to improve healthy life expectancy.
- Work with over 350 volunteers by 2025 to go the extra mile in the quality of care that we offer.
- Put patient feedback at the heart of how care is delivered in the trust, encouraging all staff to shape services around individuals’ diverse needs.
- From 2024 systematically, involve our communities at every level of decision-making in our trust throughout the year, extending our membership offer and delivering the annual priorities set by our staff and public governors.
- “Poverty proof” all our services by 2025 to tackle discrimination, including through digital exclusion.
- Deliver all ten health improvements made in the “Core20PLUS5” programme to address healthcare inequalities among children and adults: achieving 95% coverage of health checks for citizens with serious mental illness and those with learning disabilities from 2024.
- Research, create and deliver five impactful changes to inequalities faced by our population in accessing and benefitting from our autism, learning disability and mental health services as part of our wider drive to tackle inequality (the RDaSH 5).
- Consistently exceed our apprentice levy requirements from 2025, and implement from 2024 specific tailored programmes of employment access focused on refugees, citizens with learning disabilities, care leavers and those from other excluded communities.
- Be recognised by 2027 as an outstanding provider of inclusion health care, implementing National Institute for Health and Care Excellence (NICE) and NHS England (NHSE) guidance in full, in support of local Gypsy, Roma and Travellers (GRT), sex workers, prisoners, people experiencing homelessness and misusing substances, and forced migrants.
- Deliver in full the NHS commitment to veterans and those within our service communities, recognising the specific needs many have, especially for access to suitable mental health and trauma response services.
- Work with community organisations and primary care teams to better recognise and respond to the specific needs of the rural communities and villages that we serve.
- Substantially increase our Home First ethos which seeks to integrate physical and mental health provision to support residents to live well in their household, children’s home or care home, including older adults.
- Assess people referred urgently inside 48 hours from 2025 (or under four where required) and deliver a four-week maximum wait for all referrals from April 2026: maximising the use of technology and digital innovation to support our transformation.
- Support the delivery of effective integrated neighbourhood teams within each of our places in 2024 as part of our wider effort to deliver parity of esteem between physical and mental health needs.
- Focus on collating, assessing and comparing the outcomes that our services deliver, which matter to local people, and investing in improving those outcomes year on year.
- Embed our child and psychological health teams alongside schools, early years and nursery providers to help tackle poor educational and school readiness and structural inequalities.
- From 2023 invest, support and research the best models of therapeutic multi-disciplinary inpatient care, increasingly involving those with lived experience and expert carers in supporting our patients’ recovery.
- End out of area placements in 2024, as part of supporting people to be cared for as close to home as is safely possible.
- Deliver virtual care models in our mental and physical health services by 2025, providing a high quality alternative to prolonged admission.
- Actively support local primary care networks and voluntary sector representatives to improve the coordination of care provided to local residents, developing services on a hyper local basis.
- Develop consistent seven day a week service models across our intermediate care, mental health wards and hospice models from 2025 in order to improve quality of care.
- Invest in residential care projects and programmes that support long-term care outside our wards: specifically supporting expansion of community forensic, step-down and step-up services.
- Expand and improve our educational offer at undergraduate and postgraduate level, as part of supporting existing and new roles within services and teams while delivering the NHS Long Term Workforce Plan.
- Achieve Real Living Wage accreditation by 2025, whilst transitioning significantly more of our spend to local suppliers in our communities.
- Become an anti-racist organisation by 2025, as part of a wider commitment to fighting discrimination and positively promoting inclusion.
- Deliver the NHS Green Plan and match commitments made by our local authorities to achieve net zero, whilst adapting our service models to climate change.
- Extend the scale and reach of our research work every year: creating partnerships with industry and Universities that bring investment and employment to our local community.
Are we delivering our 28 promises?
Promise 1
Employ peer support workers at the heart of every service that we offer by 2027.
June 2025 update
In 2024 we invested £500,000 in expanding peer support and have done the same in 2025. Together, this significant step moves forward the scale and reach of peer support, which is now:
- embedded in children’s services within each place the trust serves
- attached to community mental health teams across Doncaster
- developing across community mental health services in both the community and acute directorates in North Lincolnshire
- available with partners in some Rotherham services
- and being introduced into some physical health service teams
During the summer and early autumn of 2025, we need to take rapid action to complete two important planning activities:
- finalising our proposals to ensure that peer support workers, whether employed by the trust or by partners, have access to suitable wellbeing support and other infrastructure to enable postholders to be effective, including within multi-disciplinary teams
- completing planning of the trajectory of posts needed to meet the promise’s success measure, recognising that a number of new and existing posts may need to be configured to reach across services locally
The trust benefits from work with community partners in developing peer support work inside the organisation, and is also working to learn from neighbouring NHS trusts who have developed such services at scale over prior years. Given the appointments made into roles since 2024, we also now have a large and capable group of peer support workers to help us think about what is needed in the future.
Key to the delivery of some other promises in this report is ensuring that all acute and older adult mental health wards within the trust have consistent access to peer support workers and governance to ensure that that occurs now in place.
Promise 1 easy read

Promise 1
Employ peer supporters at the heart of every service we offer by 2027.
- Rotherham, Doncaster and North Lincolnshire all have employed peer supporters in their children’s services.
- Peer Support Charter, focus on quality and partnership.
- Launch of a Peer Support Hub based in Doncaster as a learning model.
- Partnership working across Rotherham, Doncaster and North Lincolnshire Peer Support Community Organisations.
- 25 services across Rotherham Doncaster and North Lincolnshire included Peer Support within Investment bids.
- Doing with the communities it serves.
- Equity across Rotherham, Doncaster and North Lincolnshire.
- Increase awareness of peer support and its value, it’s more than a promise.
- Revise the understanding of the promise to make sure peer support is at the heart of every service where it is needed.
 Hello my name is Tracy and I am one of a growing number of peer support workers that are part of the trust teams. I work in The Primary Care Mental Health Hub.
Hello my name is Tracy and I am one of a growing number of peer support workers that are part of the trust teams. I work in The Primary Care Mental Health Hub.

I am employed by The People Focused Group, so this means I can keep the true values of peer support but I am also a fully integrated Rotherham, Doncaster and South Humber NHS Foundation Trust (RDaSH_ team member.
I think that this is quite a unique arrangement but it works well. Being part of a full community of peer support means that I am able to bring so much more to my role. The people don’t just get me as peer support worker they get access to a whole community.
Over the last year I have definitely seen an increase in peer supporters joining trust teams. We regularly link up and are able to provide each other with support, this is so valuable and helps us to stay well. I was one of the first peer supporters employed in this way and nearly three years on I am still here and loving every day. I have seen a real positive change in how we are all able to work together and get the best for everyone that we support.
I would definitely say that Rotherham Doncaster and South Humber NHS Foundation Trust (RDaSH) are standing up and delivering on promise 1.
The community would like to say thank you to RDaSH for doing peer support with us and not to us. The journey hasn’t always been an easy one but we have learnt lots together. The commitment to true values based commissioning is fully respected by the community it serves.
RDaSH doing what’s right and not what is easy on promise 1.

Promise 2
Support unpaid carers in our communities and among our staff, developing the resilience of neighbourhoods to improve healthy life expectancy.
Success measures
- Achieve Carers Federation accreditation for the work that we do across the trust.
- Provide flexible, safe, timely access to all our inpatient areas for carers to spend time with their loved ones.
- Identify most and better support all unpaid carers in our workforce, recognising carers traditionally excluded.
- Identify all-age carers that use our services and ensure their rights under the carers act are recognised.
June 2025 update
In early 2025, we set up a Carers’ Network to support our employees with caring responsibilities. The network will help us identify better ways to support carers through changing our policies and practice. A revised remote working policy, which will be launched in 2025, may play an important role in providing flexibility to carers. It is important to recognise all of the benefits that caring responsibilities bring to the trust’s work, acknowledging the compassion and insight into our services that can come from unpaid care.
We have not made as much progress in the last year with the support for carers of our patients. During 2025, we will make sure that carers can more easily access our wards to visit their loved ones. This standardisation of hours, permissions, and norms will need to be introduced thoughtfully because the different approaches we have developed have been for valid reasons. However, as we move to view our wards as ‘one hospital,’ we want to be able to support expectations among our communities and a reduction in unwarranted difference for staff who move between settings. We will use Care Opinion and other feedback systems to test the effectiveness of these changes that are central to our commitment to the national Culture of Care standards.
By far the most far-reaching measure of this promise is the universal adoption of processes to ensure that our practice always aims to identify, and where suitable, positively refer, carers for additional support. It is recognised that local authority-led assessment models, configured under the Carer’s Act, vary and cannot always then offer the full range of support. We will work through 2025 and 2026 to be ready to migrate to a new normal during 2026 and 2027. Within our online patient record DIALOG+ we will ensure that we ask and record patient and carer needs and preferences to secure carer assessments. The delivery plan to achieve this transition will be considered by the board in July 2025.
Promise 2 easy read

We have set up a group to help our staff who also care for a loved one outside of work.
We have got more work to do to help carers of our patients. In 2025 we will change the times that carers can visit their loved ones on our wards, so carers can come at any time.
We will also make sure that we assess, with the council, what help carers need and provide support.
Carers voices
- “I think support has changed a little in a positive way it’s easier to find support than before but more needs to be done like being available in more locations and as a side note I would like to see more SEND friendly activities that I can take all my children to together”
- “I don’t get any support and no one has ever asked me about being a carer when I take my children to appointments”
- “My mum is under the Care Home Liaison team. I was getting support as a carer with my own mental health issues. but then the worker went off sick. The manager told me they had staff shortages and I would hear from them soon, that was two months ago. In this time my mum has got more ill and my mental health has got bad”
- “I think information needs to be given out to everyone about carers as times change and we can all become a carer or the cared for sooner than we realise”
Support unpaid carers in our communities and among our staff
We spoke with 9 people that had been in contact with the trust over the last 12 months who completed a short survey. We decided then to speak to some of the carers to understand their experiences which are shared on the next page.
- Where people did receive support it was positive.
- Carers are not being identified routinely.
Were you asked about identifying a carer as part of the assessment or discussion?
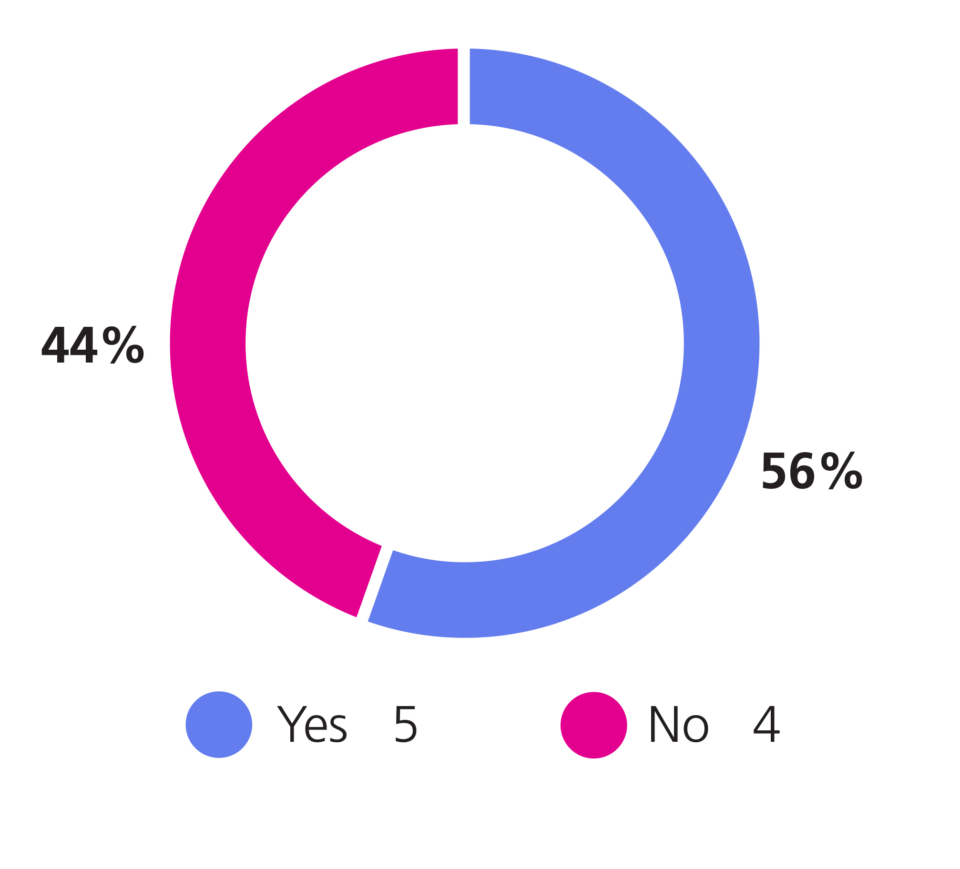
Were you provided with details about any carer support available within your own community?
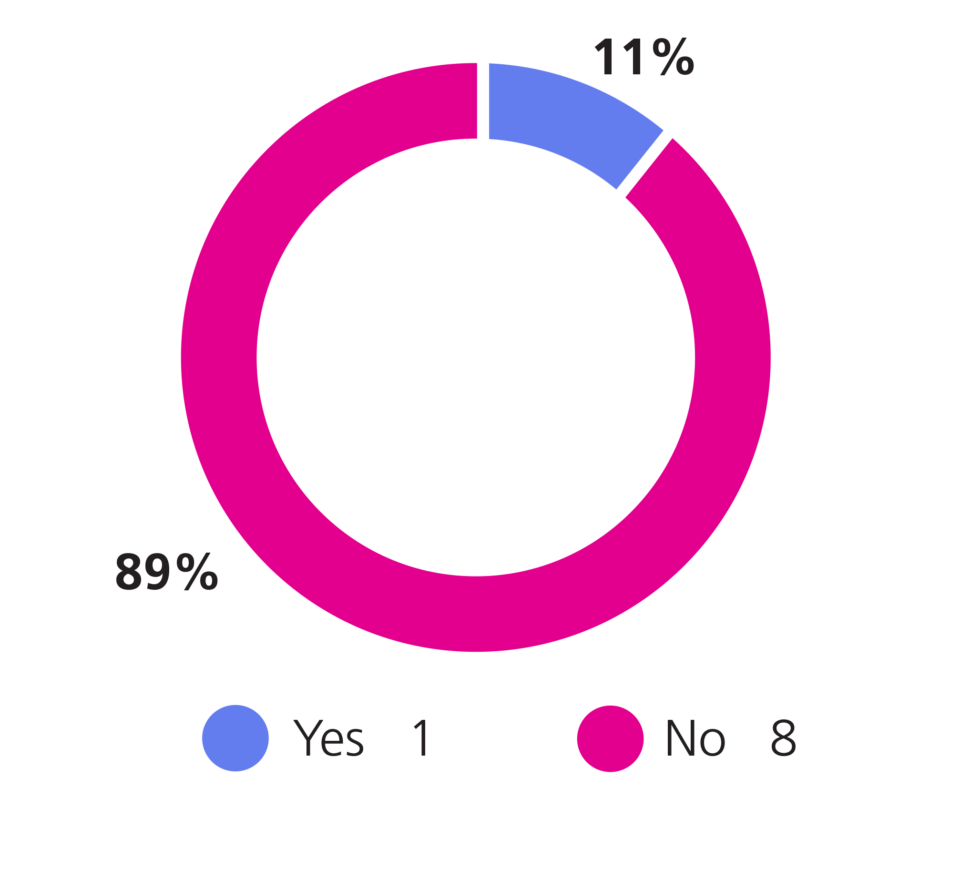
Were you provided with information about any support available for carers?
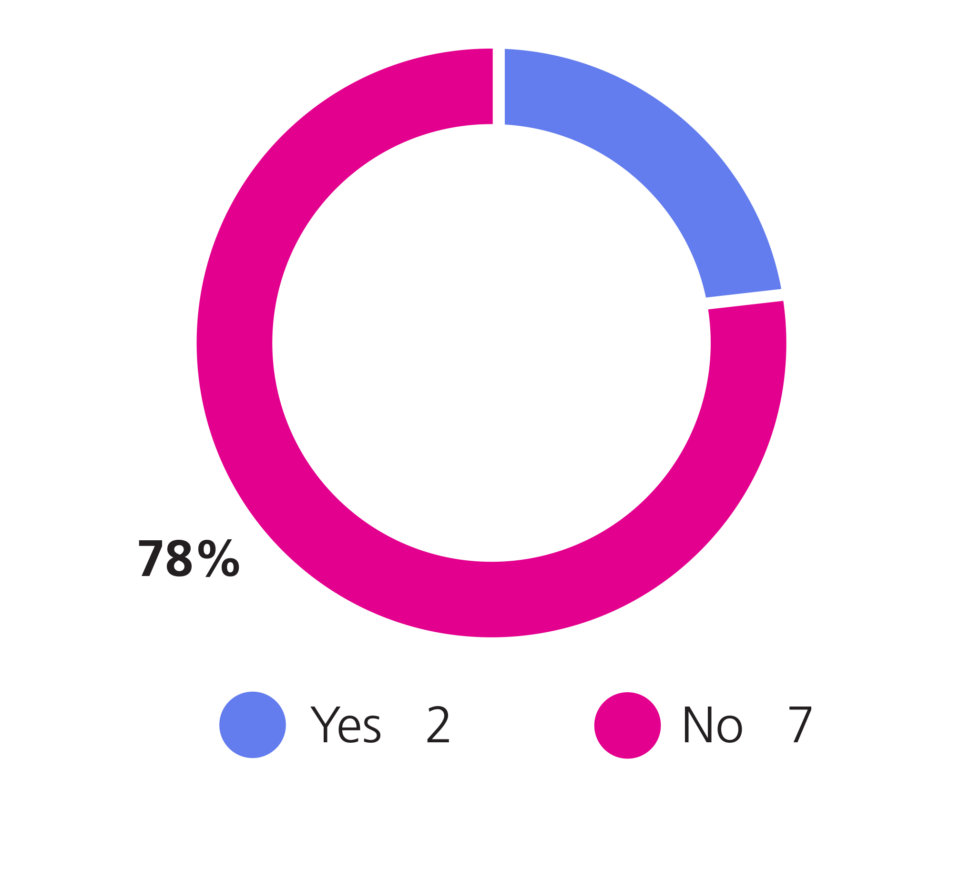
Were you asked what help or support you may need as a carer?
This is my husband Paul and I am his carer
Paul is a veteran and has multiple health conditions, these include being a right leg amputee, early onset dementia, brain injury, difficulties with his blood pressure and epilepsy. He has good days and bad days but usually manages to keep a smile on his face.

We live in North Lincolnshire and we get support from the Ironstone Centre. I have been Pauls carer for many years but recently I received a carers assessment in my own right. It felt reassuring to be recognised as a carer because I always thought I was just being a wife. There is a lot of pressure in being a carer especially when Paul’s health fluctuates so much and the future is so uncertain.
I was provided with information about local carers support and just had the chance to talk about the way I felt. Usually all of our appointments are about Paul and his needs so it was good to talk about my own.
I have been Pauls carer for many years so I can definitely say that RDaSH are living up to promise 2 as my needs as a carer have been discussed and I know where to turn to if we need more help.

Promise 3
Work with over 350 volunteers by 2025 to go the extra mile in the quality of care that we offer.
Success measures
- Have 350 volunteers registered to work with us or have equivalent to that figure volunteering time with us through another body.
- For that body of volunteers to reflect the diversity of our populations.
June 2025 update
We have made good progress recruiting volunteers in the last twelve months. However, there is urgent work taking place this summer to ensure that we meet our promise from October 2025. We have over 240 volunteers working within the trust now, as against approximately 100 in 2023. Equally importantly, those volunteers now work across a wide range of services and geographies. Our volunteers are in place across all of our geographies, many of our services, both clinical and backbone, and are adding value to our patients and teams.
Each group within the trust is expected to host at least 50 volunteers, and further expansion is needed within North Lincolnshire and Rotherham to meet this expectation. It will be crucial that this sizeable body of volunteers are able to find a collective voice. A volunteer representative sits within the Trust People Council, and during 2025 and 2026, the council of governors will review progress with volunteers and volunteering. This reflects the priority that they have given to these issues. A key part of our membership offer is to support volunteering, and all volunteers automatically become members of the trust.
We have not explicitly defined volunteer diversity. The start point reflected a female, Caucasian, older adult profile not atypical within the NHS. It is important that changes made do not dissuade these citizens from volunteering with the trust: we would expect, based on the evidence of 2024 and 2025, that younger adults, including those from minority ethnic backgrounds, may seek to join us as we expand the range of volunteering roles, and as we make clearer the pathway-into-employment that volunteering can represent. We will continue to monitor diversity by reference to both population census data and our resident population.
Promise 3 easy read

We now have a lot more volunteers in our organisation with 246 in place. We plan to have 350 by October 2025.
Volunteers are from all parts of our communities. Our volunteers are important to us and will be part of our Trust People Council so that we can listen to their views.
Work with over 350 volunteers by 2025
We asked Rotherham, Doncaster and South Humber NHS Foundation Trust who confirmed that they have 246 volunteers now in place. This means that they are on track to make this promise a reality by the end of 2025.
The community review agreed that they didn’t want to just look at numbers but they wanted to make sure that volunteering at the trust was meaningful varied and valued.
The community review talked to 8 people who have been active volunteers within the last 12 months.
Sharon Pederson and Laura Cox have shared their personal journey and experiences of volunteering on the next page. Their experiences include being part of interview panels, stakeholder events, assessing wards across Rotherham, Doncaster and North Lincolnshire, providing community support within acute wards as well as preparing plain english documents.
These two volunteers alone have clocked up 362 hours over the last 12 months!
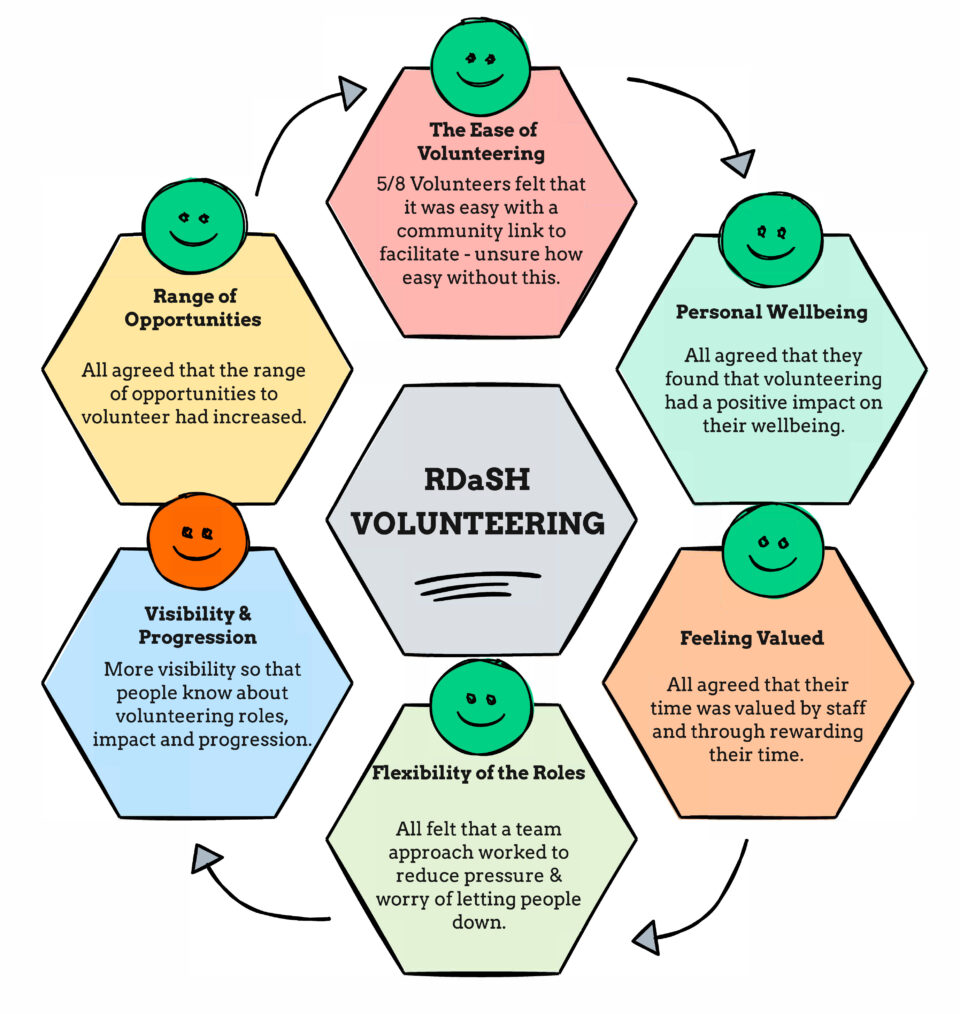
Volunteering
- The easy of volunteering: 5 out of 8 volunteers felt that it was easy with a community link facility, unsure how easy without this.
- Personal wellbeing: all agreed that they found that volunteering had a positive impact on their wellbeing.
- Feeling valued: all agreed that their time was valued by staff and through rewarding their time.
- Flexibility of the roles: all felt that a team approach worked to reduce pressure and worry of letting people down.
- Visibility and progression: more visibility so that people know about volunteering roles, impact and progression.
- Range of opportunities: all agreed that the range of opportunities to volunteer had increased.
Sharon
For the last 8 years I have been a peer supporter I have always liked helping others so when I was asked if I would like to volunteer with the trust I jumped at the chance. Through personal family experience I wanted to understand more and try to make a difference.

I find that by not wearing a uniform people open up and talk about things that they may not talk to staff about. Conversations start to flow and by being a continuous face trusts starts to build. We are able to find more information and help point people in the right direction when they are discharged.
Just getting a “cheers, see you next week” makes me feel happy and I leave with a smile on my face.
Then I was asked if I would like to do interviews at Tickhill Road. I have now done numerous interviews for staff at all levels. To know that I am putting peer support input into the interviews makes me feel proud to help and choose the right person for the job. I have been involved in unannounced visits and audits of all the wards across Doncaster, Rotherham and North Lincolnshire.
This is all part of the 28 promises and I am living proof that I feel involved and connected to the promises. I can show that I am actively involved in decision-making at all levels and I am looking forward to even more opportunities.
Laura
I would like to thank Rotherham, Doncaster and South Humber NHS Foundation Trust and People Focussed Group for giving me the chance to volunteer. It has helped me with my mental health and physical health. It has helped me with my confidence and I really enjoy volunteering on the wards.

I enjoy talking to patients and helping where I can through my own lived experience. I really enjoy being on the interview panels and was initially very shy and nervous but now I am okay and feel able to ask more questions.
I am really pleased that I have the chance to do all the things I do as a volunteer.
Promise 4
Put patient feedback at the heart of how care is delivered in the trust, encouraging all staff to shape services around individuals’ diverse needs.
Success measures
- Increase by 15% the scale of feedback received in the trust versus 2024 and 2025 baselines.
- Ensure that feedback is sought and received from a diverse range of backgrounds including those subject to Mental Health Act detention.
- Demonstrate that patient feedback at directorate level has resulted in meaningful change by 2026.
June 2025 update
The trust launched Care Opinion in the autumn of 2024, and over 1,000 stories have been shared with us since then. On average, we receive approximately 72 Care Opinion stories a month. Many stories reflect positively on the care offered by teams across the organisation. Others identify things we need to improve or directly ask for help or intervention. The stories reach directly into the organisation and are viewed and responded to by local clinicians and managers. This is important in considering the impact that stories can have on teams.
This feedback is also reaching into the processes by which the trust is managed. Consistently within the board, clinical leadership executive and within groups and directorates, both the overall impression of stories received, and their themes, and individual stories are shared and considered. They are given parity with more traditional quantitative forms of analysis.
We recognise there are some services that need additional support with patient feedback, including our forensic and learning disability services, and from people detained under the Mental Health Act. We have worked with patients to co-design a supportive feedback survey that can be used in a one-to-one conversation with a peer or completed online.
Whilst it is important that we increase the level of feedback received from our patients and carers, most importantly, we need to learn from what we are told and make improvements where required. During 2025 and 2026, we will work with colleagues at directorate level to understand better what meaningful changes have taken place in response to patient feedback. But also to understand what has been learnt that works and must be retained as the trust evolves or could be shared between teams to bring greater consistency to our care.
Promise 4 easy read
We have changed the way we ask patients and carers for feedback on their care to a system called Care Opinion. So far, 748 people have shared their stories with us online and we have responded to them. We want to make sure all of our patients are giving feedback to every service. We also need to make sure that we make changes based on what our patients tell us.
Put patient feedback at the heart of how care is delivered
Our team decided to check out this promise by firstly testing how easy it was to provide feedback across trust services.
Visited sites
Our team visited 10 areas across Rotherham Doncaster and North Lincolnshire 100% had clearly displayed information.
Phoned up
Our team made 8 phone calls across the areas and asked how they could provide feedback 100% happy with answers.
Checked online
4 members of the team checked online ability to give feedback 75% happy.
Requested paper copies
5 people during their actual appointments asked for paper copies and each received Your Opinion Counts 100%.
The community found that it is easy and well advertised to know how to give feedback in a range of ways.
Promise 5
From 2024 systematically, involve our communities at every level of decision-making in our trust throughout the year, extending our membership offer and delivering the annual priorities set by our staff and public governors.
Success measures
- Involve patient and community representatives fully in our board, executive and care group governance.
- Deliver the board’s community involvement framework in full.
- Apply patient participation tests to new policies and plans developed within the trust.
- Support active membership participation in the work of the trust, implementing a new membership offer in 2024 and 2025 and evaluating it in 2026 and 2027.
- Deliver the annual priorities set by our council of governors.
June 2025 update
During 2024, we introduced community representation into our governance structure with presence at our clinical leadership executive and all of its sub-groups.
Whilst progress has been made with community representatives forming part of board and committee work, we plan to expand this by establishing a “shadow clinical leadership executive” in summer 2025. This will be an important part of a maturity matrix that looks to develop our corporate governance model, bringing diverse patient voices into effect to help set agendas, as well as to comment on proposals developed by leadership teams. The Good Governance Institute has reviewed progress with that corporate governance model over the course of the past year, and offers independent corroboration of its development and the power within it of patient voices.
The broader community involvement framework was approved in January 2025. As we work to enhance our partnering arrangements and structure in 2025, it will be important for that framework to guide our relationships, perhaps especially with the third, or voluntary, sector at a very local level. The trust needs to be visible within our communities, in spaces and places where others naturally meet, and the confidence and capability to do that is being developed through our leadership development offer for senior leaders (which includes community partners within the curriculum).
The council of governors approved the revised membership offer at its session in March 2025. This work was rooted in engagement work undertaken in autumn 2024. Deployment of that offer and the gradual reinvigoration of the construct of membership within the trust will be an important step in spring 2025. Crucially, the trust has changed its constitution to support younger members (aged 12 and over) and to actively work alongside our youth forums and structures, within our local authorities, to hear voices from a wider group of people than previously.
The priorities set by the governing body were established in autumn 2023. They mirror closely the promises and focus attention on health promotion, on volunteers and on community participation. With changes within the governing body, during 2025 and 2026 we will need to consider again whether they have been met and adapt them to reflect the priorities governors have for the management and Board of the trust.
Promise 5 easy read
We have more people from the community taking part in our work and helping us make decisions. We are going to do more of this in more parts of our organisation to make sure patients help us make the right decisions.
Our governors asked us to work on 3 important things, helping people understand how to look after themselves, bring in more volunteers to help us and find better ways to talk to and listen to people in our communities. We will check if we have done that well in 2025.
Promise 5
Involve our communities in decision-making.
Community members sit on every one of the clinical leadership executive groups. This is currently being reviewed to create opportunities for wider community inclusion.
Community members sit on interview panels and have a say in who is employed to deliver their care and support.
Often feels like some services or staff do this better than others.
Sometimes things feel too rushed to have wider members of the community involved.
Clinical leadership executive groups
- People and Teams: promises 1, 25 ,26.
- Equality and Inclusion: promises 2, 3, 8, 9,10, 12, 17.
- Quality and Safety: promises 4, 18.
- Research and Innovation: promises 16, 28.
- Estates and Sustainability: promises 23, 27.
- Learning and Education: promise 24.
- Digital: promise 20.
- Operations and Management Group: promises 6, 7, 11, 13, 14, 15, 19, 22.
- Clinical Leadership Executive: promise 5, 21.
- Finance and Risk: promise 24.
Promise 6
Poverty proof all our services by 2025 to tackle discrimination, including through digital exclusion.
Success measures
- All our services to have completed poverty proofing and be able to evidence resultant change (including digital).
- Sustained reduction in service attendance gap (7%) in lower decile neighbourhoods.
- Benefits and debt advice access to be routine within Trust services to tackle “claims gap”.
June 2025 update
Working with a national expert organisation, Children’s North-East, we have begun poverty proofing all of our services. This focuses upon the financial barriers people face in receiving health services.
Following an initial pilot in three services in 2024 and 2025 (CAMHS in North Lincolnshire, Podiatry in Doncaster, Early Intervention in Psychosis in Rotherham), 45 services across the trust have now been poverty proofed. The full programme will conclude in summer 2026, and we will be the first trust in the country to ever poverty proof all of our work.
What matters now is the action to achieve change. And learning which changes are effective, and which are not. A baseline to demonstrate the impact of the review has been set, which is to reduce did not attend or was not bought by 7% in our most deprived areas, when compared to other areas. Our data shows us that in the more deprived areas this rate is as high as 18%. Whilst not our only measure of change, it is an important one.
Changes to how we work cannot wait for the conclusion of a trust-wide poverty proofing programme. Instead, from spring 2025, we are implementing changes arising from the initial pilot work. Benefits and debt advice services have been established with the three Citizens Advice organisations that cover Rotherham, Doncaster, and North Lincolnshire. It will be important that our support and advice is equally available to children and families to whom we offer care, and a service offer relevant to those services has now gone live. We also are investing in a patient transport fund to support patients who cannot afford to travel to and from their appointment.
Promise 6 easy read

We are checking every service to make sure that money is not a barrier to use services. We have checked 45 services so far. We can now help people with money and debt problems and help them pay for transport to get to their appointments if they don’t have the money. We hope this will mean that fewer people will miss their appointments. We need to help more people with how they use phones and tablets to look at service information and make appointments.
Promise 7
Deliver all ten health improvements made in the “Core20PLUS5” programme to address healthcare inequalities among children and adults: achieving 95% coverage of health checks for citizens with serious mental illness and those with learning disabilities from 2024.
Success measures
- Achieve measured goals for chronic obstructive pulmonary disease (COPD), hypertension, asthma, diabetes, epilepsy, oral health, and children and young people mental health by 2026 and 2027.
- Achieve learning disability and serious mental illness health check measure in 2024 and 2025 and recurrently.
June 2025 update
By the end of December 2024, over 85% of patients on our registers and caseloads for a serious mental illness had received their annual health check according. And the offer had been made to over 95%. However, like many other systems in the NHS, we have not joined up our work with that of general practice: indeed, registers of need differed. Accordingly, the Board has sought to move from April 2025 to single practice registers. This represents a major safety change, which is reflected in our risk register.
For patients with a serious mental illness, there is confidence now that we can achieve 95% of this larger group of patients during 2025 and 2026. It is worth recalling that national targets in this field are 65%. However, the gap between the trust-held dataset and the primary care-held data set is very sizeable for learning disabilities, and further consideration is needed now about how this will be approached.
The balance of promise 7 measures focusing on respiratory care for adults and mental health, oral health, epilepsy and diabetes care for children and young people will largely be achieved from the outset of 202 and 2026. A review of the data quality of the work will be undertaken to test how sustainable this position will be into the coming quarters. Care group leaders are driving forward efforts to ensure that the services involved are able to reflect on any changes needed to provision based on the experience of seeking to extend the service offer to those traditionally excluded.
Promise 7 easy read

Nearly all of our patients with a serious mental illness had an annual check on their health in 2024. Some people don’t come to RDASH services and only get help from their local doctor (GP). We need to make sure they get their check on their health every year too, especially those with a learning disability.
We are also making sure people are getting help with their health especially children and young people for things like looking after their teeth, epilepsy and mental health.
Promise 8
Research, create and deliver five impactful changes to inequalities faced by our population in accessing and benefitting from our autism, learning disability and mental health services as part of our wider drive to tackle inequality (the RDaSH 5).
Success measures
- Increase access to health checks for minority ethnic citizens with learning disabilities.
- Increase diagnostic rates for dementia among minority ethnic citizens.
- Improve access rates to talking therapies among older adults.
June 2025 update
A clear project to adopt best practice in dementia services is being established, drawing on examples from Bradford in particular. We have funded support for this work for 2025 and 2026, which is intended to improve reach into communities that do not traditionally present to primary care for memory referral. No trajectory for improvement has yet been set, but the trust is committed to improving access and awareness among our own teams, and those in general practice.
Similarly, the path to increasing by 1,500 people the volume of older adults using Talking Therapies at the trust is well-advanced. This work draws on the need of patients already using trust services and efforts to offer the service to those not referred in, for example within care homes and other settings of association. It is recognised that exclusion of older people from mental health talking therapies is a longstanding national pattern, and some experimentation may be needed to understand what sustains therapy and makes it beneficial.
In 2024 we reviewed wider work to support patients with neurodiverse needs in using trust services. This is distinct from work to tackle the appallingly long wait times experienced by children and young people, as well as adults. From that wider ten-point action plan, promise 8 focuses on ward-based environments, both the built environment and the skills and knowledge of our teams. Additional training and reflective practice time will be provided to ward-based teams recognising the likelihood that about a fifth of service users at any given time may have additional sensory and other needs.
Nationally, perinatal mental health services are not successful in reaching high risk and sometimes excluded groups. This includes families from black and minority ethnic backgrounds, as well as those parents within Inclusion Health groups. The project that will be supported within this promise aims to tackle these patterns, deliberately shifting resource through outreach work towards communities that services are not currently able to reach.
It is presently unclear whether learning disability registers within the trust and primary care reflect the ethnic origin diversity one might expect among our population. The key step is to demonstrate that they do: if this can be established, then the focus shifts to health check take-up and action. If they do not, then we will need to work with the local authority and primary care colleagues to address these gaps, which may be present in other areas of the country but should be the local reality if we work closely together.
Promise 8 easy read

We have agreed the 5 changes we need to make services better for people with learning disabilities, autism and mental illness and started work on them. They are:
- making sure that more people who are black or Asian get care from our mental health and learning disability services
- people with autism find it more comfortable when they are on our wards because of the way they are laid out and run and that staff know how to look after them
- more older people get help from our Talking Therapies service

Promise 9
Consistently exceed our apprentice levy requirements from 2025, and implement from 2024 specific tailored programmes of employment access focused on refugees, citizens with learning disabilities, care leavers and those from other excluded communities.
Success measures
- Achieve the levy requirements in 2024 and 2025 and thereafter.
- In 2024 and 2025 introduce tailored access scheme for veterans and for care leavers.
- In 2025 and 2026 introduce tailored access scheme for refugees and homeless citizens.
- In 2026 and 2027 introduce tailored access scheme for people with learning disabilities.
June 2025 update
The trust fell short of full use of our financial levy in 2024 and 2025. The Board has agreed a revised plan for the year ahead, which focuses both on entry-level apprenticeships and on mid-career roles. Fully utilising the levy remains a focus for the organisation, as we expand our training spend and work as a trust to be known for the development of our people and their teams.
In 2025, success will mean spending over £830,000 on apprenticeship qualifications. At the time of writing, we have commitments to the value of £700,000 and are working to ensure that, in particular, band 4 employees across the trust are able to access apprenticeships to close the remaining financial gap and, more importantly, invest in the careers of our people.
During 2024 and 2025, there was some good work done to prepare the ground to deliver tailored access schemes moving people into employment from specific backgrounds or circumstances. However, that work focused on making inclusive our general recruitment approach. The focus in 2025 and 2026 will be on tailored and dedicated access work for four communities listed within the success measures.
During 2025 and 2026, we will also work to put in place a programme of opportunities over the following twelve months for young adults with learning disabilities. The trust works, through our Intellectual Disabilities team, with young people of a range of ages, and our ability to support people into employment is a key intervention as people age. This work is likely to be focused on particular roles within the trust, as entry-level roles, building on learning from elsewhere in the country.
Promise 9 easy read
Not as many people in our organisation are apprentices as we would like. We have got more than before, but we have more work to do to make sure more people get the chance to learn while they work. In 2025, we will help more people with a learning disability, have worked in the army, navy or air force, are homeless or have been in care as a child, to come and work for us as an apprentice.
Promise 10
Be recognised by 2027 as an outstanding provider of inclusion health care, implementing National Institute for Health and Care Excellence (NICE) and NHS England (NHSE) guidance in full, in support of local Gypsy, Roma and Travellers (GRT), sex workers, prisoners, people experiencing homelessness and misusing substances, and forced migrants.
Success measures
- Meet standards set out in published guidance issued by NICE and NHS England (2023).
- Internal audit confirms access rates being met and feedback from specific communities corroborates that insight.
- Specific service offers in place for all or most inclusion health groups by 2027.
June 2025 update
Over the last year, a variety of adult and child-focused services have worked alongside Gypsy, Roma and Traveller (GRT) communities locally to improve our own awareness of need and to develop specific service offers. This work has been actively informed by those with lived experience.
In the last six months, we have enhanced our joint work with the Amber Project (sex workers) and with prison teams, to try and ensure that there are no barriers within our services to those needing care from within these inclusion health groups. This work builds on extensive place-wide work in Doncaster to seek to focus statutory organisations on inclusion health.
Working with the pathway organisation, we are developing a specific homeless health service proposition which we expect to see start later in 2025. This will embed alongside existing services for people experiencing homelessness but also needs to ensure that trust-led addiction and mental health services are accessible and available to those in need. Dual diagnosis must not be an exclusion from our services. This development will be crucial in moving us closer to meeting the National Institute for Health and Care Excellence (NICE) guidance standards and the real needs in our communities.
In early 2026, we will complete audit work to understand the barriers currently built into our service offer, because we need not only to have suitable specialist services in place but also to ensure that our ‘general’ offer is inclusive.
Promise 10 easy read

We have worked with a big range of our community to improve access to our services.
Promise 11
Deliver in full the NHS commitment to veterans and those within our service communities, recognising the specific needs many have, especially for access to suitable mental health and trauma response services.
Success measures
- Achieve priority access to services for veterans (closing gap between prevalent population and identified attendees).
- Introduce peer-led service support offer for local residents.
June 2025 update
The trust has renewed its accreditation, at silver level, for work in this field. The intention is not simply to be recognised as a gold standard supporter of our veteran community but also to ensure that we develop bespoke support for the voluntary sector provision that veterans themselves have created locally. Current data suggests that we see only around half as many veterans as one might expect, and we need to continue to support our services to have the specialist service pathways in place to provide timely care.
There are three steps to moving forward now with this promise.
There remains work to do to ensure that our data capture at the point of care is comprehensive. This applies to our waiting list as well as our contact points. This will allow us to confirm whether we are meeting a priority commitment. There are a range of formal alternative services for veterans and their families, as well as strong local provision that is peer-led in the voluntary sector. The trust’s expertise needs to be nested alongside that provision and is not a substitute for it. That requires our professionals to have good knowledge of that landscape, for example through learning half days.
There will be gaps in provision, and steps that the trust can take, potentially in partnership with Your Hearts and Minds, to address those gaps. The peer-led support that we would wish to see veterans have access to needs to be available across the trust landscape. In 2025 we will work to see that developed and delivered moving into 2026.
Promise 11 easy read

We have continued to have a silver award for our work on supporting veterans but we want to do more. We will do this by working with veterans in the community and listening to what they need.
We will make sure veterans get seen as soon as possible by our services and also bring in some peer support workers to help our veterans.
Promise 12
Work with community organisations and primary care teams to better recognise and respond to the specific needs of the rural communities and villages that we serve.
Success measures
- Use rural health and care proofing toolkit (National Centre for Rural Health) to identify needs and potential solutions to improving access.
- Increase digital and outreach service solutions to village communities, starting in North Lincolnshire.
June 2025 update
During 2024 and 2025, we have undertaken work to better understand the challenges faced by our rural communities. In relation to coastal rural communities, we have visited the National Centre for Rural Health and Care in Mablethorpe, who have developed services to serve this rural and coastal community. This visit provided insight into the research studies linked to the impact of living in a rural and deprived community.
We have also become a member of the National Centre for Rural Health and Care to access wider networks to share knowledge and learning as we progress this promise. We have also developed links with service leaders within Norfolk who work with deprived and rural communities. This work links to our repatriation of our patients within out-of-area placements who have previously been high-intensity users of mental health services.
Work has commenced on the development of a Rural Mobilisation Plan, including establishing planning meetings with members from across the trust. Identification of key stakeholders and representatives from all care groups and corporate services.
We have also undertaken a community (rural) asset review within North Lincolnshire and Rotherham. During the review, we identified appropriate spaces to deliver services from, with a particular focus on rural areas. Within this workstream, services have adopted community venues out of town centre locations to improve access to services.
Our Your Hearts and Mind Charity has also awarded a community grant to Humber and Wolds Rural Action to provide voluntary drivers within North Lincolnshire to support members of the rural community to access services, maintain an active lifestyle and independence and reduce social isolation.
Promise 12 easy read

We have looked at what other places do to help people who don’t live in towns or cities get healthcare, to see what we can learn. We have found more places to see patients in that are not in towns or cities so it is easier for them to get there. Now we need to agree what else we need to do to help more people, especially in North Lincolnshire.
Promise 13
Substantially increase our home first ethos, which seeks to integrate physical and mental health provision to support residents to live well in their household, children’s home, or care home, including older adults.
Success measures
- Deliver over 130 care packages through our physical health virtual ward service.
- Sustain and expand our intravenous therapy (IV) provision in out-of-hospital settings.
- Sustain and expand our Clozapine service in off ward settings.
- Take annual opportunities to transfer services to home care where safe to do so.
June 2025 update
The physical health service is now consistently delivering 60 virtual ward beds at any one time, working with partners. There have been over 2,500 people access the physical health virtual ward since it began, which has helped people leave hospital sooner and receive care in their own homes. People can now access the virtual ward from the Emergency Department as part of a step-up pathway rather than stay in hospital.
During 2025, we will provide intravenous medicine for people with heart failure as part of the virtual ward, start to use remote monitoring technology with people in their own homes, and evaluate the need for a palliative care virtual ward. We plan to employ 2 community consultant geriatricians to support the further development of the physical health virtual ward.
In Rotherham, our community clozapine service has started work in early 2025, and similar changes in Doncaster and North Lincolnshire will occur this year. The improvement in patient-reported experiences of the new service is inspiring, when contrasted to the inpatient model adopted locally over many years.
In building towards our third report in 2026 and 2027, we will consider a schedule of other specific treatments, interventions, or services where, with support and audit infrastructure in place, we can begin to move services closer to, or into, people’s homes. This should also include exploring how services might be provided differently to improve experience, and indeed attendance. Our shift of memory services in North Lincolnshire to a “one-stop” model has been notably successful in the first few months of 2025, and a similar idea sits behind pilot changes being explored within our Child and Adolescent Mental Health Service teams.
Promise 13 easy read

We have cared for many more people in their own homes in 2024. Over 2500 people in Doncaster have been able to leave hospital sooner and carry on being looked after in their homes. In 2025, we will offer more types of treatment in people’s homes which you would normally have to go to hospital for.
Promise 14
Assess people referred urgently inside 48 hours from 2025 (or under four where required) and deliver a 4-week maximum wait for all referrals from April 2026 maximising the use of technology and digital innovation to support our transformation.
Success measures
- Meet 4 hour wait standard in 2025 and 2026, where it applies.
- Meet 48 hour wait standard in 2025 and 2026 for all urgent referrals.
- Make progress to reduce waiting lists and times and close supply gap in 2024 and 2026.
- Meet 4-week standard from April 2026 across all services.
June 2025 update
Our work on assessing people referred urgently inside 48 hours from 2025 (or under 4 where required) is behind plan for achievement from 2025. Initial scoping has been conducted, which has highlighted inconsistencies with referral categorisation across services, with 34 different definitions of urgent referrals being used across services. In addition, we are not currently operating in a way that allows for triage and assessment across all services that receive urgent referrals. Options have been considered, and a clear direction of travel agreed upon for implementation in 2025 and 2026.
Huge progress has been made in all care groups regarding waiting times for routine referrals. Significant work has been undertaken to increase visibility of waiting lists, and this has supported a large piece of validation work to ensure that all waits recorded are true waits. All waiting lists are scrutinised weekly at care group level, with a weekly subgroup of the Operational Management Group (OMG) providing oversight of this process and presenting an update monthly to OMG to ensure that progress is maintained.

Child and adolescent mental health services have been the forerunners for this work. Consistently achieving and sustaining the 4-week wait will be important moving through 2025. Learning from this improvement is then being applied to other services, with a schedule of which services will reach 4-weeks when in 2025 and 2026 now available, and being actively tracked within the board.
To sustain this success, we will need to reorganise how we manage referrals into services, and decisions made about care, with appointments being confirmed inside one week. This major change in how the trust operates had to be accomplished carefully to avoid unintended consequences. From July 2025, wait times at the trust will be routinely published on our website, both to inform patients and to assist those referring into our services.
Whilst waiting times for neurodiversity diagnosis remain measured in years, clear trajectories for improvement do exist, backed by sizeable investment, we will be moving to new access arrangements for these services, which promote self-referral and reduce the need for primary care clinicians to spend time making a referral.
Promise 14 easy read

Nearly all of our children and young people now wait less than 4 weeks for their first appointment. More work will be done in 2025 to make sure that no one waits for more than 4 weeks to be seen in all of our services.
We haven’t done much yet to make sure that people referred to us urgently are seen within 48 hours, especially at weekends. We have agreed what we need to do to improve this and will be working on it in 2025 and 2026.

Promise 15
Support the delivery of effective integrated neighbourhood teams within each of our places in 2024 as part of our wider effort to deliver parity of esteem between physical and mental health needs.
Success measures
- Support development of integrated neighbourhood teams (INTs) in 2024 and 2025 in all three places.
- Restructure trust services into those INTs during 2025 and 2026.
- Evaluate and incrementally improve joint working achieved through these teams.
- Meet 5 measures of community mental health transformation agreed in 2024 at the conclusion of the community transformation national programme.
June 2025 update
The time for this promise is likely to arrive over the period from summer 2025 through the following 12 months. There is an expectation that the NHS will determine how it wishes to shift care models into more formal neighbourhood teams. With strong place partnerships in position in all three localities, the trust for children and adult services, across mental and physical healthcare, will need to determine our response. We would anticipate that new guidance will see roles moved either formally into integrated neighbourhood teams, or in relationship to integrated neighbourhood teams.
One critical factor in that journey will be the degree to which the trust and its partners begin to shift away from specialist services and towards more general services in neighbourhoods. This has implications for training and expertise, but it may be the only credible route by which caseload pressures can be managed, and through which services can genuinely be shaped by neighbourhoods. Both staff and community partners will have seen similar “shifts” previously within and related to the NHS. It will be important to draw lessons from those prior efforts, locally and nationally, and to consider carefully the counter measures to address what may not have worked in previous change models.
It is possible that an initial national focus will be quite driven by an adult physical health agenda, and in that context as a trust we need to ensure that our response is holistic and draws on the integrative benefits of a combined community and mental health service model. But those benefits will need to be demonstrated, as we have begun to explore for older adults. In advance of this guidance, it would seem premature to set out defined trust timetables, but there is a need over the later part of 2025 to begin to explore these issues with our teams.
Promise 15 easy read

We always try to make sure that our care workers work well with the voluntary and community sector, but there is more to do and there is going to be a plan nationally on how to do it. We think that plan will be shared in the summer of 2025 and when that happens, we will sit down with community partners to look at how we can make the changes that we need to. If we improve this, people will have more joined up care and won’t need to tell their story to lots of people over and over again.
Promise 16
Focus on collating, assessing, and comparing the outcomes that our services deliver, which matter to local people, and investing in improving those outcomes year on year.
Success measures
- Implement Dialog+ by 2026, collating individual outcomes from that work.
- Report and improve patient recorded outcome measures (PROMS) supported nationally.
- Ensure each trust service is reporting one local or national outcome measure by 2025 and 2026 as part of our quality plan.
June 2025 update
Making sure that our services are helping people recover or improve their health is vital. We have set out to have a measurement system in our services that allows us to do this, to assess the outcomes for patients that matter to them.
Reported outcome measures will be used across all mental health services at the trust, using an approach called DIALOG and DIALOG+, and this will be the primary measure (one local measure) used in all services where appropriate. Where DIALOG is not appropriate (that is some children’s services), these services will use Goal Based Outcomes (GBO). The trust will also be using GBO and ReQoL-10 where clinically indicated for patients, this is in line with the three outcome measures as guided by NHS England’s national outcome measures. These outcome measures will enable services to monitor patient satisfaction scores on specific elements of life and ensure consistency in holistic care, evidencing that the interventions used are right for patients using each service.
Automation and reporting of outcome measures was in place by April 2025. These reports are aligned to the reporting scheduled as required by NHS England. The report will provide evidence of patient goals, personalised care plans, increased satisfaction, and decreased satisfaction across the 8 domains in the DIALOG scale. This allows the identification of a person’s need in relation to treatment interventions or referral to another service. It also allows for gaps in service provision to be identified, thus enabling the trust to shape services to align with what patients have identified.
Demographic information aligning to patient scores given on the DIALOG scale will provide evidence of patient need across different localities, enabling services to provide specific elements of care where it is most needed, thus supporting health inequalities. The introduction of PROMs, including DIALOG+ training, will be completed by quarter 3 (2025 and 2026).
Promise 16 easy read

It is important that we know if our care and treatment has helped people. We have introduced new ways if our care and treatment work for people. Over time we will be able to tell whether our care works better for some people and communities more than others. Where this happens, we will work with communities to find out why and make the right changes.
Promise 17
Embed our child and psychological health teams alongside schools, early years and nursery providers to help tackle poor educational and school readiness and structural inequalities.
Success measures
- Narrow the school readiness gap between our most deprived communities and average in each place in which we work.
- Seek to see 80% of children meet their own potential for school readiness by 2028.
June 2025 update
During 2024, we asked parents for feedback on accessing information or advice from our health visiting teams regarding school readiness. Overall, parents found the teams helpful, particularly for advice on vaccinations, weight monitoring, head lice, diet, and general development.
However, parents also identified a need for further support in key areas such as toilet training, sleep, speech and language development, sensory issues, and emotional readiness. Challenges around behavioural difficulties, autism diagnoses, and emotional regulation were commonly highlighted, with many parents expressing a desire for additional guidance and resources to navigate these concerns effectively. Emotional readiness, particularly following the social impact of COVID-19, emerged as a key concern, alongside challenges related to diet and fussy eating. Initiatives such as school meal service stalls and literacy resource donations are helping to address these issues. Online resources, such as ERIC for toilet training and sleep support, were particularly appreciated. However, there was a clear desire for more proactive engagement from health visitors around ages 3-4 to address school readiness concerns and build parental confidence. Schools and nurseries were also recognised as key in identifying and supporting school readiness issues. Barriers to accessing support were also highlighted. These included limited awareness of available services, time constraints for working parents, lack of transport or childcare, and language barriers. Volunteer recruitment is also progressing, with the team actively seeking volunteers with relevant experience to support school readiness events. Additionally, school readiness nursery nurses have now started, enhancing the availability of direct support for families. A school readiness questionnaire has been developed and is currently being finalised, with accompanying metrics to gather robust data on outcomes.
Recruitment is also advancing for a Roma Gypsy health visitor to further enhance culturally competent support. Furthermore, ongoing discussions with the Ages and Stages Questionnaire (ASQ) provider aim to strengthen developmental screening and early intervention. Through these efforts, the health visiting team remains committed to increasing engagement, offering practical resources, and supporting families in promoting children’s readiness for school. During 2025, we will be moving to implement the changes developed by teams over the prior year. That needs to be undertaken in a manner which collects data as we go to test the impact over the following two years of the changes that we are making. It may be that this work does move the trust further away from a universalist model, and we need to recognise the choices that may come as we concentrate more resources on specific children and families. The implication of this work is that we need to use predictive tools to identify those most at risk and intervene to offer peer-led support at an earlier stage of family development.
Promise 17 easy read

We have asked parents what they think of the services we give to help their children get ready for starting school. They were happy with a lot of what we do but want more help with things like learning how to use the toilet, sleep, learning to talk and managing feelings. We are going to offer help with these things, working with volunteers and schools.
Promise 18
From 2023, invest, support, and research the best models of therapeutic multi-disciplinary inpatient care, increasingly involving those with lived experience and expert carers in supporting our patients’ recovery.
Success measures
- Meet guidance obligations from NHS England relevant to the quality of inpatient care, including safer staffing measures where they exist, and fully comply with the Mental Health Act.
- Implement programme of multi-professional quality improvement across all inpatient services by April 2026 and routinely publish data on the care provided in each environment.
- Work with patients and peers to assess the quality of services, including through peer reviews, and ensure that teams are able to act on that feedback and those evaluations.
June 2025 update
We have completed culture of care assessments of our mental health wards, informed by the voices of our patients and our staff. This work informs a visible and high-profile programme of changes within the trust, led by the high-quality therapeutic care taskforce, through which we are seeking over time to meet in full Royal College of Psychiatry accreditation standards. First steps within these changes will occur in summer 2025:
- a consistent timetable for how each of our wards will work will begin to apply across the trust
- then before winter, we will move to a daily therapeutic activities timetable, in which on every ward every day there is at least one organised and structured activity
- meanwhile, work to apply a consistent and streamlined approach to care plans is taking place, which reflects DIALOG+, and meets Care Quality Commission expectations
The move to greater consistency is intended to create space to better personalise care for patients. Under promise 8, we describe in this report moves to ensure that all our wards and ward teams feel able to support people with neurodiversity.
For staff within the trust, this is a big change in our culture and approach. Through our peer review programme, which now operates in and ‘out of’ hours, we will be able to test progress being made and consider how to adapt and evolve the standard work model we have. As far as possible, this standard work needs to reduce the administrative ask on clinical staff, liberating more time to spend with patients and working together. The trust aims to be at the forefront of its use of digital, including AI, technologies to support this work.
Therapeutic quality will come too from staff wellbeing. Reducing restrictive interventions advocates are being introduced into all of our wards, building on successful research within wards within Rotherham over the past 2 years. We want to ensure that we adopt best practice approaches, whilst reducing violence and injury experienced by staff.
Promise 18 easy read

By summer all of our wards will have the same opening hours for visitors and soon care plants will be consistent.
Promise 19
End out-of-area placements in 2024, as part of supporting people to be cared for as close to home as is safely possible.
Success measures
Cease to place patients out of their home district except where that is their choice or in their best interests.
June 2025 update
We promised in July 2023 to end out-of-area placements by December 2024. We have worked very hard to improve processes and change how we work, but we have not yet fulfilled our promise.
We have focused on improving a number of areas. This has included establishing a complex clinically ready for discharge forum with all three local authorities in October 2024, and there has been a marked improvement in all three places, with reductions in the time that patients spend in inpatient beds when they would be better cared for elsewhere, including in their own home. We have also prioritised work on the section 136 suites, with the successful introduction of a 24-hour maximum stay metric, which means suites remain open and patients are seen in a timely way. A sixth suite opened in January 2025 in Sheffield, which means more patients have access to suites in their own place, reducing pressure on other places, including Rotherham. 2024 and 2025 has seen a significant reduction in use of North Lincolnshire’s suite by patients brought from South Yorkshire.
In February 2025, we established the high quality therapeutic care task force. This will require a focus on what happens while in an inpatient setting and especially addressing length of stay, achieving the national benchmark of an average of 32 days across all the adult mental health wards. We will continue to focus on safe discharges and reducing extended stays when patients are ready to return to their communities. We will also focus on admissions, to be able to consider where safe and therapeutically appropriate community alternatives can be considered. This will require close work with systems partners; better use of our “crisis houses” and continued investment in rehabilitation services across all places. This work is intended to allow the trust to accommodate 16 additional patients each month in our care, which should help us to cease to make use in almost all cases of out-of-area placement for acute patients. We have not used out-of-area beds for older adults during 2024 and 2025, and our plans for these services are based on this position remaining unchanged.
In October 2025, we open a high dependency unit at Tickhill Road, serving patients across North Lincolnshire and South Yorkshire. This unit will allow more than a dozen long-term out-of-area placements to be supported in our communities. If this development is successful, we may extend and expand to a second unit over the coming 2 years.
Promise 19 easy read

We know that sending patients away from their home towns for in-patient care is not good for the patient or their families. We set out to stop this happening by December 2024 but we haven’t managed to do this. A lot of work is happening to look at what happens when you are an in-patient so that your stay is useful, how long you need to stay and help people get back home as soon as possible.
This work should start to mean that fewer people need to be sent away from their hometown for care, but there is still a lot to do to make this happen
Promise 20
Deliver virtual care models in our mental and physical health services by 2025, providing a high-quality alternative to prolonged admission.
Success measures
- Deliver over 130 care packages through our physical health virtual ward service working with partners.
- Introduce and evaluate virtual ward pilot into our mental health services 2024 and 2025.
- Introduce and evaluate virtual ward pilot within our children’s services 2025 and 2026.
June 2025 update
The trust is contributing to analysis of virtual ward pilots for children’s services across South Yorkshire before determining how to adopt our own service. In older people’s mental healthcare, summer 2025 will see the trust begin our own pilot in North Lincolnshire to explore the potential of virtual ward provision.
The “physical” health service virtual ward has been established for some time. It is now consistently delivering 60 virtual ward beds at any one time, working with partners. There have been over 2,500 people who have accessed the service since it began, which has helped people leave hospital sooner and receive care in their own homes. Over the last year, we have made changes, with partners, so that people can now access the virtual ward from the Emergency Department as part of a step-up pathway rather than only after a stay in hospital.
With the adoption of our digital enabling plan in summer 2025 and given the anticipated emphasis of the NHS 10-Year Plan, we hope to see further growth in these service offers during the coming year. Virtual offers can significantly empower patients to have much greater control over their care but also their wider life, and this aim is important to us as we look to focus on outcomes that matter to patients.
Promise 20 easy read

We have cared for many more people in their own homes in 2024. Over 2500 people in Doncaster have been able to leave hospital sooner and carry on being looked after in their homes. In 2025, we will offer more types of treatment in people’s homes which you would normally have to go to hospital for.

Promise 21
Actively support local primary care networks and voluntary sector representatives to improve the coordination of care provided to local residents, developing services on a hyper-local base.
Success measures
- Fulfil our commitment to support a community first model working alongside partners in South Scunthorpe: focusing first on those with serious mental illness.
- Contribute actively to the city-wide Thrive programme within Doncaster, using a liberated method to ensure that duplication and handoffs of care are reduced.
- Implement anticipatory preventive care models supported within the Rotherham Place programme, where possible using such approaches to reduce demand for secondary care.
- Understand and act on local research into patterns of referral, cross referral and best fit services for mental health in adults and older adults linked to general practice.
- Consistently integrate our community mental health offer with that provided by voluntary sector organisations, sharing training, data and expertise to improve outcomes.
June 2025 update
Starting work on this promise was delayed in 2024 while we worked with partners in each place to best understand what mattered to other agencies. The success measures were adopted early in 2025 and reflect those conversations.
Building on patient feedback in the annual members’ meeting of 2024, we are working with Primary Care Doncaster on a formal study of patterns of referral, declined referral, and transfer between primary care facing mental health services. Investment in such services has been extensive since 2019, but it remains the case that patients can feel “left in limbo”. We are exploring how we can more actively assess a “best fit” service for patients from those we provide and avoid, or end, requests to primary care to re-refer people into different teams. Our GP liaison lead has worked extensively with over 50 local practices to understand their experiences of our current arrangements as we look to develop alternative approaches within neighbourhoods.
In each place there are different approaches to this neighbourhood working, and RDaSH is active in each collaboration. What they have in common is a need to focus on continuity and those at highest need. This demands better approaches to sharing data and to sharing expertise, including, and perhaps particularly with local voluntary sector enterprises (VCSE). Investing in the VCSE sector remains a priority for the Trust corporately, as it is for our charitable foundation which has committed grants to over 30 local organisations this year.
Promise 21 easy read

We believe that giving people care and treatment closer to their homes is better. We also think we need to do this with others such as the local doctor, chemist, social worker etc. We have been working with others to see how we can do this better and are training up our managers to work more closely with communities. It is important for us to work with voluntary organisations to meet the needs of communities and we will do more of this in 2025.
Promise 22
Develop consistent 7-day-a-week service models across our intermediate care, mental health wards, and hospice models from 2025 in order to improve the quality of care.
Success measures
- Ensure that access to urgent and emergency services is equitably available through Saturday and Sunday (this must include crisis and safe space availability).
- Support substantially increased discharge and admission capacity over weekends.
- Assess and publish during 2025 an analysis of quality and safety risks specific to our pattern of weekend working in key services.
June 2025 update
During 2024, we have not made progress on this promise. However, the high quality therapeutic inpatient care (HQTC) task force was set up in February 2025. This will focus on meaningful admissions, safe discharges, and a therapeutic care model on all wards. There is recognition that we currently admit to our inpatient wards at weekends but do not discharge, which will be part of this work. We will want to learn from other trusts who do conduct 7-day discharges, or, for example, undertake diagnostic-led discharges, and consider how they utilise community services to work differently, partners such as the local authority, and utilise the voluntary sector. We will also need to extend in-hours practice, so there is bed availability going into weekends and capacity.
The trust has invested to support Safe Space provision. This has been, in Doncaster, now integrated with our statutory services, with shared data access. Our aim is clear that such services are best led through the voluntary sector, but that integration in a practical sense is critical.
The Board will receive an analysis of the quality and safety issues arising from a typically five-day model during summer 2025. We will look to explore these issues alongside colleagues within local mental health, learning disability, and autism collaboratives. There is recognition that not everything can be offered on every day across a seven-day week, but that we may need to alter working patterns and invest to improve care outcomes. In particular, we need to ensure, as indicated within promise 14, that urgent access is available when needed.
There is work at an early stage, currently, to examine how using digital solutions, we might extend access to children’s urgent care through weekends. This is likely to be a proposal for system funding on a trial basis in 2026.
Promise 22 easy read

We know it is important for people to be able to access the same level of care 7 days a week. We haven’t done as much on this during 2024 as planned. In 2025 we will ask our wards to discharge patients at weekend, look at what care is provided on wards at the weekend and offer some of our children’s services online 7 days a week.
Promise 23
Invest in residential care projects and programmes that support long-term care outside our wards, specifically supporting the expansion of community forensic, step-down and step-up services.
Success measures
- Develop bed-based mental health services within each of our communities by 2028, as additions or alternatives to ward-based practice: ideally delivering these services through partner organisations.
- Expand the scale of our residential forensic rehabilitation service.
- Establish and support a step-up service for older peoples’ care in Doncaster by 2027.
June 2025 update
Work to expand Danescourt within our forensic service is ready to implement once Care Quality Commission accreditation is confirmed this summer. This will improve access and allow more local support and is part of wider efforts to ensure that community rehabilitation is sufficiently scaled to meet local needs. Retaining local connection is especially important for these services and this client group, where isolation and stigma can be acute.
We have worked with partners to develop our proposals for older people’s care in Doncaster, the city’s Health and Wellbeing Board has prioritised this project as part of their wider work to support living and ageing well. Site plans are being finalised for the initial development which we expect to see start construction in early 2026. The development is a key part of work create alternatives to Emergency Department attendance, offering so-called step-up capacity which can support avoiding longer term acute admission. This capacity is an important part of the place plan to address long waits in Emergency Department and delays in transferring patients from ambulances. The trust’s work with care homes is especially significant to these improved pathways.
We have worked in partnership with South Yorkshire Housing to open a 10-unit residential property (Burns Court, Rotherham) to support patients with a serious mental illness to step down from complex rehabilitation placements. This is focused on returning patients from out of area into their own flat with a tenancy. Clinical support for this scheme is provided through trust teams including assertive outreach. During 2025 we plan to offer tenancy properties to patients with a serious mental illness in partnership with St Leger Homes in Doncaster, probably in Bentley, and discussions with partners across North Lincolnshire are also taking place.
It will be important that developments of this nature become part of, rather than add-ons to, the clinical pathways and services that the trust provides. Over the previous decade the trust has been part of similar initiatives at times, and that connection and inclusivity has proved elusive. The scale of what is being attempted now is larger than before, and there is visibility across the clinical leadership executive, of the work which must support reducing use of more traditional inpatient services.
Promise 23 easy read

Sometimes people need support to live in the community rather than staying in hospital. We have opened a place in Rotherham which has 10 separate flats so that people can move in for a short while with support from their health team and housing teams. We plan to do the same in Doncaster and North Lincolnshire in 2025 and 2026.
Promise 24
Expand and improve our educational offer at undergraduate and postgraduate level, as part of supporting existing and new roles within services and teams while delivering the NHS Long Term Workforce Plan and step-up services.
Success measures
- Student feedback to reach upper quintile when compared to peers.
- Trust workforce plan for 2028 on track to be delivered.
- Trust meets expectations applied through national Long Term Workforce Plan roll out.
June 2025 update
The trust has a ring-fenced training budget, and that is now spent in line with local teams’ training plans. Data on the equity by protected characteristic of that spend is analysed as part of the management of education in the organisation.
This approach is also taken to releasing time to learn. From September 2024, learning half days have created dedicated monthly time for this purpose, where colleagues, students and volunteers across the organisation can engage in a range of opportunities for formal or informal learning and quality improvement work. During 2025, we are working to expand this offer to better support those working shifts on a weekend or overnight basis.
In all professions, we are undertaking a renewed “job plan” exercise to ensure that time is provided for learning and continuous professional development, alongside supporting the contribution to research and formal education that we expect of senior clinicians within the trust.
Recruitment and retention plans in the organisation are ahead of our initially anticipated timescale, with the move to being “fully staffed” being achieved in April 2025. Sustaining that position will of course require constant attention and vigilance, not least as new roles are created and new teams like our High Dependency Unit. Reducing turnover will help us, and there are early signs of progress with that endeavour.
Feedback from students remains very positive, and external accreditation measures continue to show us meeting our success measures. A review of this in respect of social work roles is imminent.
The trust wants to be known as better than the NHS norm for its work on education and learning. There are encouraging signs that both inputs to that end, and perceptions among existing and potential staff, are moving us closer to that aim.
Promise 24 easy read

We have set aside money for training and our staff have half learning days every month. Our students say nice things about us, we were fully staffed by April and our staff are staying working with us.
Promise 25
Achieve Real Living Wage accreditation by 2025, whilst transitioning significantly more of our spend to local suppliers in our communities.
Success measures
- Obtain Real Living Wage Foundation accreditation in first half of 2025.
- Pay the Real Living Wage to our own employees from April 2025, or sooner.
- Transfer more of our spend to local suppliers (shift of 25% or more compared to 2023 and 2024).
June 2025 update
In April 2025, we paid the Real Living Wage. This changed take home pay for colleagues working on bands 2 and some on band 3, who the NHS pays below the Real Living Wage elsewhere. This practical step will make a real difference for employees. Colleagues like domestic workers (often cleaning and serving food for patients) have seen their wages rise. The Real Living Wage is independently set with a new rate announced each November and paid from the following April.
We hope to be accredited as a Real Living Wage employer during July 2025. This reflects not only our changes in pay policy but also work to ensure that we contract and buy from organisations that also achieve fair pay. Over the previous 12 months, we have worked with our suppliers to test their pay policies, and where necessary, move contracts to those that do. Procurement activities now require, as a qualifying matter, suppliers to confirm that they pay above the Real Living Wage hourly rate.
A radius of 25 miles from our main care sites is being considered to be local. The trust is moving our supply chain to seek to be within that radius for much of what we purchase, that is not covered by the wider collaborative buying arrangements of the NHS. Changes in 2025, will complete the transition in accordance with our initial measure of success. We want to continue, partnering with Rotherham Council and the social value portal to ensure that we invest time and attention in the local supply chain, their ability to work with us, and ours with them.
We recognise that, even with these major changes in place, hardship continues, and individuals may find themselves facing debt or other difficulties. Specific grant relief funding is available to employees, and projects like our free period and sanitary products, and food cupboards, are in place now across the trust.
Promise 25 easy read

It is important that all our staff can afford to live, and some of them were paid below the real living wage, which is an amount of pay that helps people afford their bills, food, and transport. We have now increased the pay for those staff, which is helping them. We are also working with people we get to do jobs for us, like building work, to see if they are paying their staff the Real Living Wage to help people employed in our communities.
Promise 26
Become an anti-racist organisation by 2025, as part of a wider commitment to fighting discrimination and positively promoting inclusion.
Success measures
- Implement suite of policies and practice to kick racism out of our trust.
- Tackle and eliminate our workforce race equality standard (WRES) gap by 2026.
- Receive credible accreditation against frameworks of inclusion for all excluded protected characteristics, starting with global majority.
- Tackle our gender pay gap.
June 2025 update
In 2024, we agreed our plan to tackle racism in our organisation. The adoption and implementation of our acceptable behaviour policy allowed us to have a consistent approach to warning, and where necessary, excluding from care or site access, individuals unable to apply our standards of reasonable conduct. In responding to the August 2024 riots, especially in Rotherham, the trust acted to support staff and students, and to address any involvement by our employees.
The 7-point plan to address racism has been actively implemented over the year. For example, any allegations of racism inside the trust between employees are now investigated by an individual from a global majority background. This is intended to build confidence and help colleagues in the trust, to trust the formal processes that we apply. Our recruitment data now suggests that a much larger cohort than before are drawn from Black and Minority Ethnic backgrounds, as we seek to reflect the communities in which we work.
Our WRES data does show improvement against the prior year in reducing the number of staff facing discrimination. But the position remains unacceptable, and continued work to address micro-aggressions, and to support all staff to be allies, continues. Senior leaders have completed specialist training with Mokita and equality diversity and inclusion objectives are in place for board members.
Focusing on the gender pay gap and benefitting from the move to the Real Living Wage, the trust has largely closed the gap, which at one juncture reached 11%. The wider anti-discrimination work of the trust includes action to tackle employment and retention barriers for staff with long-term conditions or disabilities. Considerable investment has taken place, but we know from staff survey and Workforce Disability Equality Standard (WDES) information, that we are not yet outstanding. The board is working alongside our staff networks to ensure that practical steps are taken to improve, and that the voices of those with lived experience are heard and lead our conversations. This shift is “owned” or led through the trust People Council, which was created in the last year to support changes to the culture of the trust.
Promise 26 easy read

We are working hard to reduce racism at the trust, close the pay difference between men and women and have introduced the Real Living Wage, meaning staff who were on lower wages are now better off.
Promise 27
Deliver the NHS Green Plan and match commitments made by our local authorities to achieve net zero, whilst adapting our service models to climate change.
Success measures
- Reduce our carbon tonnage by 2000 (and offset balance).
- Agree and deliver specific contribution to local authority climate change plans.
- Change service models for patients and staff to reduce travel required by 2027.
June 2025 update
We understand what is needed to meet our promise. The scale of change involved, and the funding requirement is, of course, significant. The biggest step required of the organisation is to reduce our dependence on gas as an energy source because this is creating the most carbon emissions. Propositions to move to new technologies such as heat pumps are contingent on funding streams and on our wider estate plans.
During the first half of 2025, we will develop proposals that could be funded on this basis and look to move the retained estate within our Tickhill Road site, as a priority, to these revised methods by the end of this decade, if not by 2028. In developing our estate, we need to take opportunities to update the heat retention and wider energy efficiency of our buildings. This will help us to reduce cost and waste.
As a trust our services and our staff teams are spread across an extensive geography. In most cases, there is not a credible travel alternative to the use of individual cars. There are opportunities to plan our services with a reduced travel footprint, both in how we schedule our service and where we base our teams. These opportunities will be useful to us and active consideration of them needs to be explored as teams develop their plans for 2026 and 2027. The prime opportunity remains for the trust a more systematic approach to remote working. The revised policy will need to bring forward a fair, service-relevant, model that supports roles to have some time outside the workplace, without sacrificing team working, training, line management and supervision, or access for patients.
As part of our work to meet a wider environmental and sustainability commitment, the trust continues efforts to reduce single-use items, including plastics. This work is led and supported through our network of green champions. It will be important that this distributed enthusiasm for the work that we need to do is developed and supported as the Trust looks to meet its commitment over the lifetime of the strategy.
Promise 27 easy read

A lot of our buildings are heated by using gas and this is harmful to the planet. There are ways to heat buildings which don’t use gas, and we are putting together plans to try to get some money from the government to pay for this. We also need to find ways for our community to staff to drive less so they are not harming the planet. This will be difficult because we need to see patients in their own homes, but we could manage it better. We have also stopped using things that we throw away after we’ve only used them once like plastic cups.
Promise 28
Extend the scale and reach of our research work every year, creating partnerships with industry and universities that bring investment and employment to our local community.
Success measures
- Meet portfolio study recruitment targets each year.
- Deliver metrics contained in the trust’s research and innovation plan.
- Work to further increase the reach of research into excluded communities locally.
June 2025 update
The trust has once again, through the hard work of clinicians and our Grounded Research team, achieved the study targets set for us. This means that over 1,000 people have been entered into trials.
As an organisation, we have sought to measure the quality of our research systems and processes and be held to account in terms of the best standards globally. To that end, we have proactively put ourselves through the inspection processes set out by the International Accrediting Organisation for Clinical Research (IAOCR), at 2 levels. One in relation to a site accreditation, and the second in relation to workforce accreditation. We have achieved Gold Standard in each category.
We have consistently championed patient and public engagement in the design and delivery of all its research and innovation work. As well as having a number of active public contributors helping us both on the ground in individual studies, we have sought to go further in relation to inclusion in research with a number of leading-edge examples. Two such examples are our sponsorship of the Physical and Mental Health of Older Prisoners (PAMHOP) trial with the University of York, which focuses on the mental health of older prisoners, and our successful bid to host the Ethnic Minority Research Inclusion network for the region.
The development of our partnership to support specialist research into the appropriate use of psychedelic treatments, will be an important step over the coming year. Likewise, our work on the 6 research priorities that the board has agreed, an initial focus on dementia will see us expand our trial activity and seek to actively recruit clinicians with a research interest in this field. We continue to undertake research and evaluation of our strategy itself, including to build a better understanding of health check strategies and effects in patients with serious mental illness.
Promise 28 easy read

We have had a lot of people taking part in research and trials and we have been recognised for our work.
Tell us what you think of us, of this report, and let us know what matters to you in the year ahead…
We want to hear from you. Your feedback will directly inform the work of our ‘shadow’ clinical leadership executive, whose role is outlined in the introduction to this report. We will use your views to help shape our agenda, and to test whether our promises are being delivered in practice.
You can contact us in any of the 5 ways outlined below, whichever makes sense to you:
- through Care Opinion
- via our partner (People Focused Group), email: hello@peoplefocusedgroup.org.uk
- using our corporate Communications team, email: rdash.rdashcommunications@nhs.net
- through our lead governor Jo Cox, email: joan.cox7@nhs.net
- direct to the trust’s chief executive on behalf of the board, email: tobylewis@nhs.net
We are especially interested to listen to, and talk with, you about your experience of any of our promises. That is because we do not want to “deliver” the success measures of our promise but miss the point. Only by hearing about your experiences of what works, and what does not, will we learn and adapt.
When we closed our report last year, we hoped to make progress with 10 of our promises over the coming 12 months. In closing the report this year, we need to openly reflect on delivery of that expectation.
This report confirms that 7 of those 10 have moved substantially forward:
- we have invested another £500,000 in peer support (promise 1)
- we are on track to deliver on expanding volunteering (promise 3)
- poverty proofing is now embedded in how we work (promise 6)
- we have expanded apprenticeships and have a clear plan to meet the levy expectation in 2025 (promise 9)
- waiting times are reducing towards four weeks (promise 14)
- clinical teams are working hard to improve inpatient care (promise 18)
- we are paying the Real Living Wage (promise 25)
That means 3 promises are less advanced, each difficult in their own way. Working on neighbourhood health needs to accelerate (promise 15), the excellent start we have made with DIALOG+ training needs to convert into widespread use and then used to analyse outcomes (promise 16) and, as a trust, we need to work with partners to improve 7-day, and specifically, weekend working and access (promise 22).
The board of the trust is unequivocal. We will keep working to deliver these promises and to turn nurturing the power in our communities into the “day job’.
A big thank you to the People Focused Group (PFG) who have provided easy read throughout the document and given their input on our promises 1 to 5, which sit under objective 1 which covers nurturing partnerships with patients and citizens to support good health.
Page last reviewed: January 16, 2026
Next review due: January 16, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem