1 Introduction
Domestic abuse is a pervasive societal issue, impacting individuals across all demographics, irrespective of sex, ethnicity, class, religion, sexuality, or disability. It constitutes a fundamental breach of human rights. While the trust acknowledges that the majority of victims and survivors are female, this policy adopts a gender-neutral definition to ensure inclusivity and comprehensive support for all. Domestic abuse can occur in any type of personal relationship. The trust recognises that patients, colleagues, volunteers, and contractors may be affected by domestic abuse in various ways, as a victim or survivor, living in an abusive relationship, or as a perpetrator. The overarching aim of this policy is to promote the health, safety, and wellbeing of everyone interacting with the organisation. Multi-agency partnership working is crucial for effectively addressing domestic abuse at both operational and strategic levels. The trust actively participates in strategic partnerships across localities, demonstrating its commitment to responding effectively to domestic violence and abuse. Research consistently demonstrates the profound impact of domestic abuse on individuals’ mental and physical health. This policy serves as a resource for colleagues when domestic abuse is disclosed, outlining available support mechanisms and procedures.
2 Purpose
This policy provides a framework for the trust colleagues to confidently and competently identify and respond to domestic abuse in adults, young people, and children. It covers both victims and survivors and perpetrators and provides support for colleagues experiencing domestic abuse. It aligns with all relevant UK legislation and policy, including the Human Rights Act (1998), Children Act (1989 and 2004), Care Act (2014), Domestic Abuse Act (2021), Data Protection Act (2018), National Institute for Health and Care Excellence guidelines (2016) and Department of Health (2017).
3 Risk factors
Adapted from Office for National Statistics (ONS) and national guidance.
Clinicians must be aware of the following high-risk factors:
- victim’s perception of risk: victims often underestimate the danger to themselves, children, and others
- separation or child contact: leaving an abusive relationship can escalate the risk of serious harm, including homicide; child custody disputes are often a trigger
- pregnancy and or new birth (child under 18 months): abuse can begin or intensify during pregnancy and after childbirth
- escalation and or repeated violence: the frequency and severity of abuse often increase over time
- community issues and or isolation: specific needs of diverse communities (ethnic minorities, newly arrived communities, asylum seekers, older people, people with disabilities, travellers, LGBTQ+ individuals) must be considered, including potential for forced marriage and honour-based violence; isolation and vulnerability can be significant factors
- stalking: persistent and consistent calling, texting, following, and other forms of harassment are strongly associated with serious harm, including homicide; stalking reflects fixation and obsession
- coercive control and or extreme jealousy: complete control over the victim’s activities and extreme jealousy are red flags for serious violence and homicide, honor-based violence must be considered, perpetrators may attempt to control professionals
- strangulation or choking or suffocation or drowning: these are particularly high-risk indicators of lethal violence
- mental health and substance misuse: while not the cause of abuse, these can be contributing factors and may exacerbate the situation
- child abuse: actual or witnessed child abuse requires mandatory reporting to relevant services
- animal abuse: a known link exists between animal abuse and domestic abuse
- suicide-homicide: perpetrators’ threats of suicide are linked to homicide in abusive relationships
4 Prevalence of domestic abuse
Office for National Statistics (ONS) Data year ending March 2024.
The following data is drawn from the Office for National Statistics (ONS) publication Domestic abuse in England and Wales overview: November 2024 (ONS, 2024). It is crucial to acknowledge that these figures, while representing the best available data, may still underestimate the true prevalence of domestic abuse due to underreporting and the limitations of survey methodologies.
4.1 Overall prevalence
In the year ending March 2024, an estimated 2.3 million adults aged 16 and over in England and Wales experienced domestic abuse. This represents 4.8% of all adults
4.2 Gender breakdown
The prevalence of domestic abuse varies significantly by gender:
- an estimated 1.6 million women (6.6% of women) experienced domestic abuse
- an estimated 712,000 men (3.0% of men) experienced domestic abuse
4.3 Trends
- Recent trend: there was no statistically significant change in the prevalence of domestic abuse in the year ending March 2024 compared with the previous year.
- Long-term trend: while there has been no recent change, the prevalence of domestic abuse has shown a gradual decrease over the last 10 years, from 6.5% in the year ending March 2014.
- Types of abuse: a higher percentage of adults experienced domestic abuse by a partner or ex-partner (3.2%) than by another family member (1.9%).
- Lifetime prevalence: approximately one in five (20.5%) adults in England and Wales have experienced domestic abuse since the age of 16.
5 Domestic abuse related death reviews (DARDR)
Domestic abuse related death reviews (DARDR) are multi-agency reviews of deaths (aged 16 and over) where domestic abuse is suspected to be a factor (Domestic Violence, Crime and Victims Act 2004). They aim to identify systemic failings and improve responses to prevent future tragedies.
6 Scope
This policy applies to those colleagues that are directly employed by the trust and for whom the trust has legal responsibility.
For those colleagues covered by a letter of authority or honorary contract or work experience this policy is also applicable whilst undertaking duties on behalf of the trust or working on trust premises and forms part of their arrangements with NHS commissioners within Doncaster, Rotherham and North Lincolnshire.
As part of good employment practice, agency workers are also required to abide by trust policies and procedures, as appropriate, to ensure their health, safety and welfare whilst undertaking work for the trust.
For further information about responsibilities, accountabilities and duties of all colleagues, please see appendix A.
7 Legal framework and definitions
| Term | Definition |
|---|---|
| Domestic Abuse Act (2021) | This landmark legislation provides a statutory definition of domestic abuse, establishes the office of Domestic Abuse Commissioner, prohibits offenders from cross-examining victims in family courts, creates domestic abuse protection notices (DAPNs) and orders (DAPOs), provides a statutory basis for the Domestic Violence Disclosure Scheme (Clare’s Law), criminalises controlling or coercive behaviour (in Northern Ireland, with similar provisions elsewhere in the UK), creates a statutory presumption that victims are eligible for special measures in criminal courts, enables polygraph testing for offenders post-release, places duties on local authorities regarding support and accommodation, and requires local authorities to grant new secure tenancies to social tenants leaving existing tenancies due to domestic abuse. |
| Domestic abuse | Domestic abuse occurs between two people aged 16 or over who are “personally connected”. This connection includes:
Abusive behaviour encompasses any of the following:
It can consist of a single incident or a course of conduct. |
| Children as victims | Domestic abuse is considered to have occurred if a child sees, hears, or experiences the effects of abusive behaviour between people who are “related to” the child. “Related to” means being a parent of, or having parental responsibility for, the child, or being a relative. |
| Controlling or Coercive Behaviour (Serious Crime Act 2015) | Controlling behaviour is a range of acts designed to make a person subordinate and or dependent by isolating them, exploiting their resources, depriving them of independence, and regulating their everyday behaviour. Coercive behaviour is a continuing act or pattern of assault, threats, humiliation, intimidation, or other abuse used to harm, punish, or frighten the victim. |
8 Procedure
8.1 Key principles
- Prioritise safety: the immediate safety of the victim survivor and any children is paramount.
- Empowerment and choice: respect the victim’s autonomy and involve them in decision-making whenever possible.
- Confidentiality: maintain confidentiality within legal and ethical boundaries.
- Information and support: provide comprehensive information about available support services.
- Multi-agency working: collaborate effectively with other agencies to ensure a coordinated response.
- Training and competency: ensure colleagues receive regular training on domestic abuse, risk assessment, and relevant procedures.
- Support for colleagues: provide support and resources for colleagues experiencing domestic abuse.
8.2 Asking the question
Routinely inquire about domestic abuse as part of the clinical assessment process, when it is safe and appropriate to do so. Explain the reasons for asking and assure confidentiality. Document the outcome of the inquiry clearly and sensitively in the patient’s record. Examples: “I routinely ask all my patients about their safety at home. Sometimes people experience difficulties in their relationships. Is this something you’d be comfortable talking about today?”, “Do you feel safe at home?”, “Are you afraid of your partner or anyone else in your family?”, “Has anyone ever physically hurt you?”, “Do you feel controlled or isolated?”.
8.3 Responding to risk
Upon disclosure, colleagues must complete a domestic abuse, stalking and honour based violence risk checklist (DASH) to assess the level of risk. This is a mandatory step. Actions taken will be guided by the level of risk and the individual’s wishes, within legal and safeguarding frameworks. Consent is essential unless there is a significant and immediate risk to the individual or a child, or the individual lacks the capacity to consent. Colleagues must follow the domestic abuse disclosure flowchart (appendix C) precisely.
8.3.1 Standard risk (1 to 6 ticks)
Colleagues must provide information about local and national support services (appendix E), including helplines, websites, and refuges. Colleagues should offer assistance in contacting these services if the individual wishes. Colleagues should consider a referral to Early Help services for any children in the household. Colleagues must follow local safeguarding children and adults procedures. Colleagues must document all actions taken, including the domestic abuse, stalking and honour based violence risk checklist score, information provided, and any referrals made
8.3.2 Medium risk (7 to 13 ticks)
Colleagues must provide information about support services (appendix E) and actively assist the individual in contacting them if requested. Colleagues must seek explicit consent for information sharing with relevant agencies. If children or adults at risk are involved, colleagues must follow local safeguarding children and adults procedures. Colleagues must document all actions, including attempts to gain consent and any information shared
8.3.3 High risk (14 and over ticks or professional judgment)
If there is an immediate risk, colleagues must call 999. Colleagues must refer the case to the multi-agency risk assessment conference (MARAC) following local procedures, even if the individual refuses consent. The reasons for sharing information without consent must be clearly documented on the MARAC referral form. If children or adults at risk are involved, colleagues must follow local safeguarding children and adults procedures and make a referral to children’s social care and or adult safeguarding. Colleagues must complete an incident report
8.4 Multi-agency risk assessment conference (MARAC)
Domestic abuse incidents assessed as “high risk” using the domestic abuse, stalking and honour based violence risk checklist will be addressed through the multi-agency risk assessment conference (MARAC). MARACs are meetings where agencies share information about high-risk domestic abuse victims. A risk-focused safety plan is created to support the victim and reduce the risk to them and any children. MARAC operates on the principle that no single agency has the complete picture, but all may have crucial insights. The victim does not attend but is represented by an Independent Domestic Violence Advocate (IDVA).
Aims of multi-agency risk assessment conference:
- increase the safety, health, and wellbeing of victims and their children
- jointly construct and implement a risk management plan
- reduce repeat victimisation
- improve agency accountability
- identify situations requiring child protection procedures
- improve support for victims in high-risk cases
Multi-agency risk assessment conference membership: agencies represented typically include police, social care, 0 to 19 service, substance misuse services, domestic abuse services, education welfare, National Probation Service, mental health services, and youth offending teams
Confidentiality: under no circumstances should the perpetrator be informed of a MARAC referral. This includes subject access requests, which must be handled with extreme caution and in consultation with legal advisors
Please see multi agency risk assessment conference (MARAC) procedure for further information.
8.5 Information sharing
Any information sharing must be in accordance with the Data Protection Act (2018) (GDPR) and related trust policies. Information can be shared without consent in the following circumstances:
- where there is a risk of serious harm to the victim, any children involved, or another person
- when it is in the best interests of a person who lacks the capacity to consent to disclosure
- when the courts request information about a specific case
If in doubt about information sharing, colleagues must contact the Caldicott Guardian (medical director) or the information governance team for guidance.
9 Domestic abuse and safeguarding children
Children may suffer both directly and indirectly in households where there is domestic abuse. Hearing or seeing the ill-treatment of another constitutes harm. A referral must be made to local authority children and young people’s services if a child lives in a household where domestic violence is believed to be a factor, potentially leading to them being in need of support or protection. This referral is in addition to any actions taken regarding the adult victim or survivor. Colleagues must be familiar with and follow local safeguarding children procedures. Document all observations and concerns regarding the child’s welfare.
10 Perpetrators
The Respect phone 0808 802 4040 provides confidential support for perpetrators seeking to change their abusive behaviour. The trust recognises that addressing perpetrator behaviour is crucial for preventing future abuse. Colleagues should be aware of this resource and be prepared to provide information to individuals who express a desire to change. Local authorities may also offer perpetrator programmes; information about these can usually be found on their websites. It is important to emphasise to perpetrators that their behaviour is their responsibility and that help is available.
11 Domestic Violence Disclosure Scheme (DVDS) Claire’s law
The Domestic Violence Disclosure Scheme (DVDS) allows individuals to request information about a partner’s past history of violence or abuse. This scheme operates through two pathways: “Right to Ask” (initiated by a member of the public) and “Right to Know” (initiated by the police). If you believe someone is at risk and could be eligible for a disclosure, refer them to the police (101). Be familiar with the DVDS guidance and procedures. Remember that disclosures are made by the police, not by healthcare professionals.
12 Safety advice
Discuss safety planning with victims and survivors, emphasising that leaving an abusive relationship can be a particularly dangerous time. Offer practical advice, including:
- emergency contact: dial 999 in an emergency and teach children to do the same, ensure they know their full name, address, and telephone number
- escape plan: develop and rehearse an escape plan, including safe places to go and how to leave quickly
- emergency bag: pack an emergency bag with essential items (documents, medication, money, clothes) and keep it hidden in a safe place (not at the home if possible)
- trusted contacts: identify trusted neighbours, friends, or family members who can be contacted in an emergency, inform them of the situation and ask for their help
- financial resources: keep some money readily available, including change for phone calls and transportation
- mobile phone: keep a mobile phone charged and readily accessible
- documentation: keep records of abusive incidents, if safe to do so
13 Colleagues experiencing domestic abuse
The trust is committed to supporting colleagues experiencing domestic abuse. A separate confidential guidance document (appendix G) is available for managers and colleagues, outlining internal support mechanisms, confidential reporting routes, and links to external resources. This guidance emphasises that colleagues experiencing domestic abuse will be treated with sensitivity and respect. It also clarifies roles and responsibilities in providing support.
14 Documentation
Meticulous and accurate documentation is essential. Colleagues must:
- ensure that the electronic record is completed using the safeguarding templates on SystmOne, adhering to the records management policy. Include details of disclosures, risk assessments (DASH), actions taken, referrals made, and any safety planning discussions
- complete incident reports, adhering to the incident management policy, in all cases of suspected or disclosed domestic abuse, especially when there is a risk to children or vulnerable adults
15 Training implications
People experiencing domestic abuse should expect colleagues to respond consistently and appropriately. Training colleagues to respond to disclosure (level 1) and how to ask about domestic violence and abuse (level 2) is essential for safe enquiry about experiences of domestic violence and abuse and a consistent and appropriate response. National Institute for Health and Care Excellence Quality Standard 116 (2016) recommends levels of domestic abuse training commensurate to job role as below:
Level 1 colleagues should be trained to respond to a disclosure of domestic abuse sensitively and be able to direct people to specialist services. This level of training is for allied health professionals, healthcare assistants and receptionists.
Level 2 colleagues should be trained to undertake routine enquiry about domestic abuse in a way that makes it easier for people to disclose it. Colleagues should also be able to respond with empathy and understanding, assess someone’s immediate safety and offer referral to specialist services. This level of training is for nurses, doctors, prison staff and alcohol and drug misuse workers.
Level 3 colleagues should be trained to identify and assess risk, safety plan and liaise with specialist services. This level of training is for safeguarding children health professionals, multi agency risk assessment conference (MARAC) representatives and adult safeguarding representatives.
Level 4 colleagues should be trained to give expert advice and support for people experiencing domestic abuse. This level of training is for domestic abuse navigators.
15.1 All trust colleagues
- How often should this be undertaken: at the trust induction and 3 yearly.
- Level: basic awareness.
- Delivery method: leaflet.
- Training delivered by whom: leaflet within induction booklet and sent out three yearly by Learning and Development team.
- Where are the records of attendance held: electronic staff record (ESR).
15.2 All trust colleagues who have patient contact
- How often should this be undertaken: 3 yearly.
- Level: 1.
- Delivery method: e-learning.
- Training delivered by whom: electronic staff record (ESR).
- Where are the records of attendance held: electronic staff record (ESR).
15.3 Clinicians required to complete a dash risk assessment in response to disclosure of domestic abuse
- How often should this be undertaken: 3 yearly.
- Level: 2.
- Delivery method: face to face or virtual or e-learning.
- Training delivered by whom: external training providers.
- Where are the records of attendance held: electronic staff record (ESR).
15.4 Clinicians who may made a referral and present a case at the multi agency risk assessment conference
- How often should this be undertaken: 3 yearly.
- Level: 3.
- Delivery method: face to face or virtual or e-learning.
- Training delivered by whom: external training providers.
- Where are the records of attendance held: colleagues are required to input training on the portal.
16 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
16.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
Consequently, the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity, and respect, (when appropriate this should also include how same sex accommodation is provided).
16.1.1 Indicate how this will be met
No issues have been identified in relation to this policy.
16.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all colleagues working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason, all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005)to ensure that the rights of individual are protected, and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
16.2.1 Indicate how this will be achieved
All individuals involved in the implementation of this policy should do so in accordance with the principles of the Mental Capacity Act (2005).
17 Links to any other associated documents
- Safeguarding adults policy
- Safeguarding children policy
- Multi agency risk assessment conference (MARAC) procedure
- Health record keeping standards and health records management policy
- Clinical risk assessment and management policy
- Information governance policy
- Safeguarding principles and the approach for South Yorkshire
- North Lincolnshire multi agency policy and procedures
- Incident management policy
18 References
- Department for Health (2017) Responding to Domestic Abuse- A Resource for Health Professionals
- HM Government (1989) Children Act
- HM Government (1998) Human Rights Act
- HM Government (2004) Children Act
- HM Government (2004) Domestic Violence, Crime and Victims Act
- HM Government (2014) Care Act
- HM Government (2018) Data Protection Act
- HM Government (2021) Domestic abuse Act
- NICE (2016) Domestic Violence and Abuse
- Office for National Statistics (2024). Domestic abuse in England and Wales overview: November 2024.
19 Appendices
19.1 Appendix A responsibilities, accountabilities and duties
19.1.1 Chief executive
The chief executive retains overall responsibility for the development and implementation of trust policies.
19.1.2 Director of nursing and allied health professionals
Is the executive lead for safeguarding.
19.1.3 Deputy director of nursing and allied health professionals
The deputy director of nursing is responsible for the development, review and monitoring of this policy.
19.1.4 Head of safeguarding
- The head of safeguarding fulfils the role of corporate lead for adult and children safeguarding.
- Responsible for promoting compliance with regulatory and commissioning standards and ensuring that safeguarding policies, procedures are up-to-date and embedded within all clinical areas.
- Takes the lead on specialist areas of safeguarding practice within the trust including the Prevent agenda, domestic abuse, female genital mutilation and perplexing presentations, fabricated or induced illness.
19.1.5 Safeguarding team
- Will provide expert advice, guidance and leadership regarding domestic abuse in the context of children, young people and adults at risk.
- Deliver training around identifying domestic abuse including the impact on children as part of the safeguarding learning and development programme.
19.1.6 Multi agency risk assessment conference (MARAC) representatives
Those with appropriate training will be responsible for attending the scheduled multi agency risk assessment conference (MARAC), soliciting and disseminating information in support of the process and offering appropriate advice to colleagues regarding disclosures of domestic abuse that may form the basis of a MARAC referral.
19.1.7 Line managers
- Ensure all colleagues under their supervision have access basic awareness training on domestic abuse.
- Ensure all colleagues completing clinical risk assessments routinely ask about domestic abuse and will access relevant domestic abuse training in accordance with Responding to Domestic Abuse: A Resource for Health Professionals (DOH, 2017).
- Ensure that colleagues are trained to undertake domestic abuse stalking and honour based abuse (violence) (Dash) risk assessments.
- To be aware of the local multi agency risk assessment conference (MARAC) referral process.
- Ensure they are able to offer the initial and appropriate advice to colleagues experiencing domestic abuse. See appendix C.
- Provide the appropriate support to colleagues who have domestic abuse disclosed to them.
19.1.8 Modern matrons, ward managers and deputies and team managers
- Ensure that safeguarding adults boards and local safeguarding children board policies and procedures in relation to domestic violence or abuse are implemented.
- Ensure all colleagues attend mandatory training.
19.1.9 Safeguarding children and adult supervisors
- Inform colleagues through the supervision process of the relevance and impact of domestic violence in relation to safeguarding children and adults.
- Advise on the need for referral and action to protect the child or children and adults.
19.1.10 Human resources
Offer informed advice and confidential support, to those colleagues experiencing domestic abuse and to facilitate appropriate support mechanisms to diminish the risk of further abuse, while they are at work.
19.1.11 Clinical colleagues
- Attend training as per trust requirement.
- All clinical colleagues will receive domestic abuse information as part of their induction (basic awareness) and complete any. additional domestic abuse training as prescribed by their training matrix within 6 months (see training implications below).
- As part of the assessment process clinical colleagues are responsible for making enquiries and asking about domestic abuse.
- They will have attended domestic abuse training up to level 3 dependent on role.
19.2 Appendix B monitoring arrangements
19.2.1 Raise the question re domestic abuse as part of assessments
- How: Domestic abuse audit.
- Who by: Safeguarding team.
- Reported to: Safeguarding and Mental Capacity Act Operational Group.
- Frequency: Annually.
19.2.2 Meeting the agreed standard for training attendance for domestic abuse
- How: training compliance reported through care group dashboards.
- Who by: care group nurse directors.
- Reported to: Safeguarding and Mental Capacity Act Operational Group.
- Frequency: Monthly.
19.3 Appendix C monitoring arrangements
The trust recognises that domestic abuse is a serious issue and that incidents of domestic abuse are common and critically affect many people’s lives. The impact on a colleague experiencing domestic abuse is significant, but this may be an area that line managers are unclear about in terms of how to support the colleagues and the extent to which this is a personal or work-related area.
The effects of domestic abuse can influence the health and self-confidence of colleagues who may in turn feel unable to confide in others or seek help. Many of those that experience domestic abuse have difficulty attending work regularly and demonstrate longer term symptoms such as depression, anxiety, or stress that consequently affect work performance.
The trust recognises that it is important to increase awareness of domestic abuse and its impact in the workplace and are committed to providing guidance for both managers and colleagues and create safe opportunities and environments for disclosure.
The trust is committed to treating people with dignity and respect in accordance with the Equality Act (2010) and Human Rights Act (1998). Due regard has been given to the elimination of unlawful discrimination, harassment and victimisation as cited in the Equality Act (2010).
The trust has a duty of care and health and safety laws ensure workers have the right to work in a safe environment where risks to health and well-being are considered and dealt with efficiently.
There are four main areas of health and safety law relevant to violence at work:
- Health and Safety at Work Act (1974)
- Management of Health and Safety at Work Regulations (1992)
- Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (1995)
- Health and Safety (consultation with colleagues) Regulations (1996)
19.3.1 Confidentiality and right to privacy
- The trust has provided safe areas (known as “wobble” rooms) where colleagues can arrange to meet in private and away from their normal working area.
- Colleagues who disclose they are experiencing abuse can be assured that the information they provide is confidential and will not be shared with other colleagues without their permission.
- There are, however, some circumstances in which confidentiality cannot be assured. These occur when there are concerns about children or vulnerable adults or where the employer needs to act to protect the safety of colleagues.
- In circumstances where there needs to be a breach of confidentiality, specialist advice and support will be sought before doing so, keeping the colleagues informed and ideally gaining their consent. Information will only be shared on a strict need-to-know basis.
- All records concerning domestic abuse will be kept strictly confidential. No local records will be kept of absences related to domestic abuse and there will be no adverse impact on the employment records of victims or survivors of domestic abuse.
19.3.2 Recognising the indicators that point towards a problem with domestic abuse
Domestic abuse is often associated with physical violence, but it can also be emotional or psychological (please see definitions in main body of domestic abuse policy).
The below indicators may point towards a problem of domestic abuse, but they could also be the result of a different issue such as ill health. An aware and proactive manager and colleague should be looking out for these issues more generally as an indicator that something might be wrong, without assuming it will be related to domestic abuse.
The more supportive atmosphere we can create as an employer, the more likely our colleagues are going to feel comfortable disclosing a problem with domestic abuse.
19.3.2.1 Work productivity
- Change in work patters, for example frequent absences.
- Change in quality and quantity of work for example drop in usual performance.
- Changes in phone and email usage for example avoiding calls or strong reactions to calls or emails.
- Increasing number of hours at work for no reason.
- Change in partners behaviour, for example frequent visits to work, which may indicate coercive control.
19.3.2.2 Physical indicators
- Visible bruising or repeated injury with unlikely explanations.
- Change in pattern or amount of makeup used.
- Change in manner of dress for example clothes that do not suit the climate which may be used to hide injuries.
- Substance use or misuse.
19.3.2.3 Changes in behaviour or demeanour
- Conduct out of character.
- Changes in behaviour for example quiet, anxious tearful, aggressive.
- Isolating from colleagues.
- Obsessed with leaving on time.
- Secretive about home life.
19.3.2.4 Other indicators
- Partner or ex-partner stalking colleague in or around the workplace or on social media.
- Partner or ex-partner exerting unusual amount of control or demands.
19.3.3 Raising the issue
Colleagues experiencing domestic abuse may want to consider informing their employer. It is recognised that this is not always an easy step for those experiencing domestic abuse.
However, any disclosure will be respected and confidentiality will be maintained if at all possible.
Colleagues who are trade union members may also wish to contact their staff-side representative to access trade union support.
In the first instance colleagues are encouraged to inform their line manager if they are experiencing domestic abuse. In this regard, managers will take disclosure seriously, consider the information fully and sympathetically, recognise that admission can be a difficult experience and, where appropriate, seek advice from human resources.
In some cases, colleagues may prefer to raise their concerns with someone other than their line manager (either direct or indirect). If this is the case colleagues can contact human resources directly in confidence.
19.3.4 If a manager sees signs of domestic abuse
If a manager sees signs that a colleague is experiencing domestic abuse then a meeting should be facilitated as soon as possible to discuss their concerns and identify appropriate support:
- suggest that you go somewhere quiet and comfortable, away from their workplace
- support the colleague
- have an open posture
- be prepared for them to be upset and tearful
19.3.5 Responding to a disclosure
Managers should respond promptly in providing a non-judgemental and supportive environment to ensure the colleague feels safe when disclosing. This includes respecting their boundaries and privacy.
It is important to be clear that it is not the manager’s role to deal with incidents of domestic abuse or advise colleagues on dealing with domestic abuse but assist the colleague to enable them to decide on a suitable course of action. The manager should:
- provide a sensitive and non-judgemental approach
- ensure that confidentiality is respected as far as possible
- recognise that the colleague may need some time to decide what to do and may try many different options during this process
- discuss measures to prioritise safety in the workplace
- complete a Dash assessment with the individual to identify the level of risk
- be aware of what support is available and explore these options with the colleague. The trust can offer support from the employee assistance programme (03303 800 658, available 24 hours a day)
- provide information for specialist domestic abuse services
- consideration should be given of the impact on any children in the relationship and referral to children’s social care
- managers should keep a written note of discussions as they may be required as evidence, any information should be stored confidentially within the colleagues personal file
19.3.6 Risk assessments
If domestic abuse is disclosed, undertaking a workplace risk assessment can ensure that the potential risk to colleagues and colleagues is lessened. It is important to note that each person’s needs are different and that any measures should only be used with the authorisation or consent of the individual concerned. Risk assessments may also assist the manager to offer suitable support.
This may include:
- paid or unpaid leave to attend relevant appointments, (with support agencies, solicitors, to rearrange housing or childcare, or at court)
- temporary or permanent changes to working times and patterns
- changes to specific duties, for example to avoid potential contact with an abuser
- temporary redeployment or relocation
- measures to ensure a safe working environment, for example changing a telephone number to avoid harassing phone calls
- using other existing policies, including flexible working
- access to counselling or support services in paid time
- temporary onsite parking
- each case will be considered on its merits and managers and colleagues should agree on a combination of annual leave, flexitime and paid or unpaid absence; where agreement cannot be reached, managers have the right to treat this as sickness absence
19.3.7 What not to do
Don't
- do not advise a colleague to leave their partner as this may place them at higher risk
- do not ask the colleague if they wish to “make a complaint or prosecution”, this is a police and Crown Prosecution Service decision
- do not ask the colleague why they stay
- do not suggest that a colleague work from home on a regular basis, just ask what they would prefer
19.3.8 Safety planning
The trust will actively provide support to colleagues to minimise the risk to their safety while at work. A workplace risk assessment should be considered with the assistance of the trusts head of security and line manager;
- closed circuit television (CCTV) is available on most trust premises
- colleagues have access to personal alarms
- lighting has been improved in all public areas of the trust
- reminders not to divulge information about colleagues, especially personal details
- offering temporary changes to workplace, work times and patterns to reduce the risk at work and journeys to and from work
- blocking emails
- changing work phone numbers
- escorting colleagues off premises
- provision of safe places within the trusts service areas (“wobble” rooms)
- in extreme cases provide safe accommodation
19.3.9 Perpetrators of domestic abuse
Domestic abuse perpetrated by colleagues will not be condoned under any circumstances nor will it be treated as a purely private matter. The trust recognises that it has a role in encouraging and supporting colleagues to address violent and abusive behaviour of all kinds.
Domestic abuse is a serious issue which may lead to criminal proceedings. In these circumstances, management reserves the right to conduct its own internal inquiry using the trust procedure for managing allegations against people in positions of trust (PiPoT).
Managers must escalate to the safeguarding team and HR department when an incident occurs that may warrant investigation and disciplinary action and ensure that the matter is progressed through the stages of this procedure in a consistent and timely manner.
If the victim and the perpetrator are both colleagues, the human resources department should be contacted so that appropriate action can be considered. Action will depend on individual circumstances but could include:
- temporary adjustments to duties and or location of one or both colleagues
- potential action under the disciplinary policy
- advice from and or involvement of the police
In addition, adult and child safeguarding policies should be considered if a manager becomes aware that a colleague is potentially or actually perpetrating domestic abuse and may seek advice from the safeguarding team.
Domestic abuse is always the responsibility of the perpetrator, however, managers should aim to support colleagues undertaking action to address their behaviour associated with perpetrating domestic abuse, taking account always of the trust responsibility to protect children and adults at risk.
19.3.10 Local resources
All resources regarding domestic abuse can be found on safe guarding adults domestic abuse (staff access only) on the trust intranet.
19.4 Appendix D domestic abuse flowchart
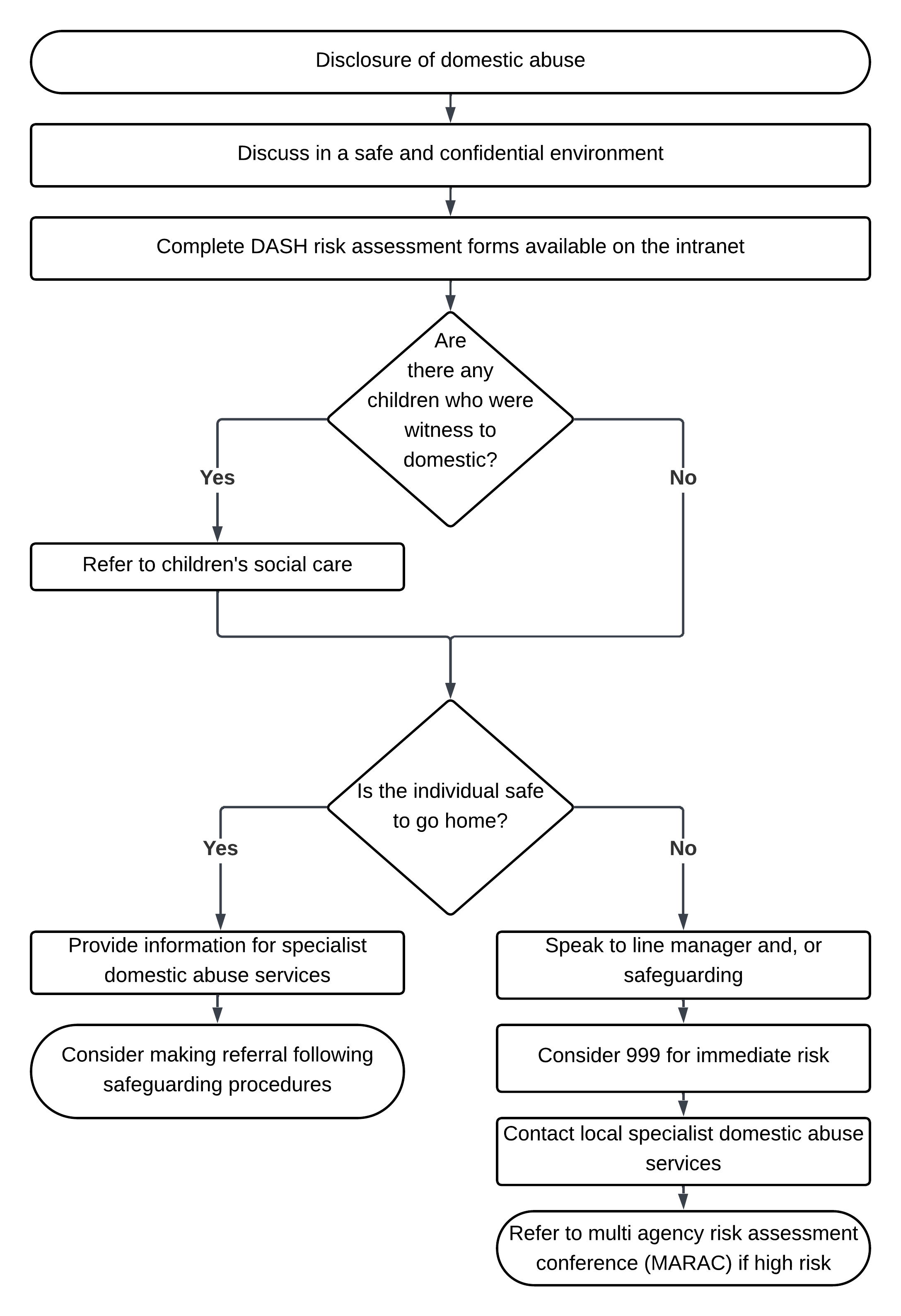
- Disclosure of domestic abuse.
- Discuss in a safe and confidential environment.
- Complete DASH risk assessment forms available (staff access only).
- Are there any children who were witness to domestic?
- If yes, refer to children’s social care.
- Is the individual safe to go home?
- If yes:
- provide information for specialist domestic abuse services
- consider making referral following safeguarding procedures.
- If no:
- speak to line manager and, or safeguarding
- consider 999 for immediate risk
- contact local specialist domestic abuse services
- refer to multi agency risk assessment conference (MARAC) if high risk
- If yes:
Note, if circumstances suggest police intervention is urgent and necessary, call 999.
Remember don’t act as a domestic abuse care worker for the person once you have referred the individual. However, if involved with the individual you may form part of the risk management.
19.4.1 Risk levels
High risk: refer to multi agency risk assessment conference (MARAC), consent not required.
Medium risk: provide information for local and national domestic abuse services.
Low risk: provide information for local and national domestic abuse services.
19.5 Appendix E support services
19.5.1 Doncaster
-
- Women’s aid: Advice helpline 01302 326 411. A confidential advice service is available by face to face appointments or over the phone.
- Doncaster domestic abuse hub, at the safer Doncaster partnership: 01302 737 080.
- Multi agency domestic abuse services: single point of contact for male and female services: 01302 326 411 (Doncaster Women’s Aid).
19.5.2 Rotherham
-
- Women’s refuge (by Rotherham rise), Rotherham, open Monday to Friday from 9am to 5pm: 0800 470 1505
- Choices and options: 01709 838 400
- Apna Haq: 01709 519 211
- Independent domestic violence advisor service: 01709 823 981
- Rotherham rise: 0330 202 0571
19.5.3 North Lincolnshire
-
- Independent domestic violence advisor service based at the It’s my right project: 01724 841 947
- Women’s aid, Grimsby: 01472 575 757
- Blue door: 0800 197 4787
19.5.4 National helplines
-
- Male victims of domestic violence: 01823 334 224
- National domestic abuse helpline (free phone run by Refuge): 0808 2000 247
- The men’s advice line, for male domestic abuse survivors (run by Respect): 0808 801 0327
- The mix, free information and support for under 25s in the UK: 0808 808 4994
- National LGBT+ domestic abuse helpline (run by Galop): 0800 999 5428
- Live free from fear helpline (run by Welsh women’s aid this helpline supports men and women and provides support in English and Welsh): 0808 801 0800
- Samaritans (24 hours and 7 days service): 116 123
- Mankind: 01823 334 244
Respect, lead on the development of safe, effective work with perpetrators, male victims, and young people using violence in their close relationships.
Further information is available on the safeguarding intranet page
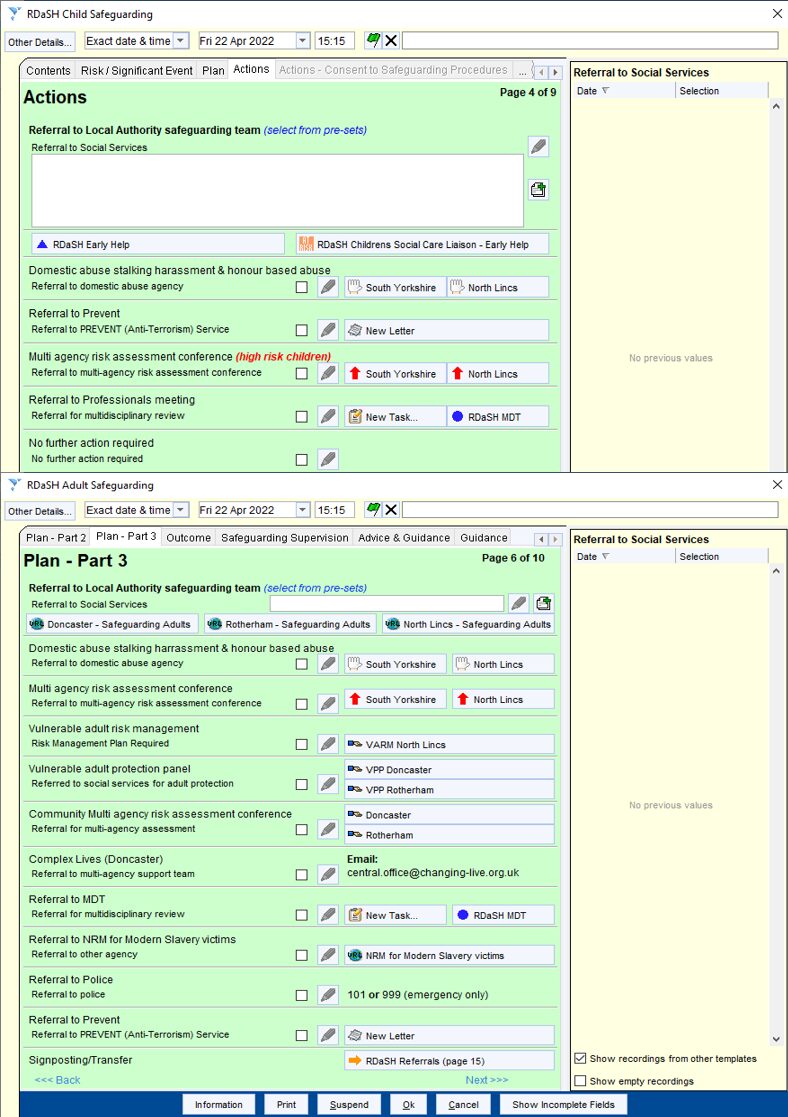
19.6 Appendix F SystmOne templates for safeguarding
19.7 Appendix G guidance for supporting colleagues experiencing domestic abuse
Refer to appendix G: guidance for supporting colleagues experiencing domestic abuse (staff access only).
Document control
- Version: 8.1.
- Unique reference number: 152.
- Approved by: clinical effectiveness meeting
- Date approved: 13 May 2025.
- Name of originator or author: head of safeguarding.
- Name of responsible individual: chief nursing officer.
- Date issued: 18 June 2025.
- Review date: 30 June 2028.
- Target audience: all staff within the organisation.
Page last reviewed: June 26, 2026
Next review due: June 26, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.