1 Policy summary
Female genital mutilation (FGM) is defined as any procedure that involves the partial or total removal of the external female genitalia, or any other injury to the female genital organs for non-medical reasons. This practice is often referred to by various terms, including female circumcision, cutting, initiation, or Sunna (HM Government, 2020). It is crucial to recognise that female genital mutilation is not a religious practice, but rather a deeply ingrained social norm in specific communities.
The prevalence of female genital mutilation is concentrated in 30 countries, primarily located along the Atlantic coast of Africa, the Horn of Africa, parts of the Middle East, and some regions in Asia. In England and Wales, it is estimated that approximately 103,000 women aged 15 to 49, and 24,000 women aged 50 and over, who have migrated from these countries, are living with the consequences of female genital mutilation. Additionally, it is believed that around 10,000 girls under the age of 15, who have also migrated, have likely undergone female genital mutilation. However, the true extent of female genital mutilation within the UK remains unknown due to its hidden nature and the reluctance of individuals to disclose their experiences.
Female genital mutilation is often perpetuated by families and communities due to complex social and cultural beliefs. It is frequently perceived as a necessary rite of passage for girls to become accepted as women and to be considered marriageable. This misconception is a crucial factor in the persistence of the practice. It is vital to reiterate that female genital mutilation is an unacceptable practice, devoid of any justification, and constitutes a severe form of violence and child abuse. Healthcare professionals have a statutory obligation, under national safeguarding protocols such as Working Together to Safeguard Children (2023), to protect children and adults who are at risk of, or have undergone, female genital mutilation.
2 Introduction
The multi-agency statutory guidance on female genital mutilation (HM Government, 2020) provides a framework for agencies to collaborate in protecting and supporting those affected by female genital mutilation. This policy is designed to be used in conjunction with that guidance, ensuring that cases are managed within existing child protection and adult safeguarding structures.
To effectively protect and support individuals at risk or who have undergone female genital mutilation, all agencies must adhere to the following principles:
- paramount safety and welfare: the safety and welfare of the child must be the primary consideration in all actions and decisions
- rights of the child: all agencies must act in accordance with the rights of the child, as outlined in the United Nations Convention on the Rights of the Child (1989)
- illegality of female genital mutilation: female genital mutilation is illegal in the UK, and this legal status must be clearly understood and communicated
- harmful nature of female genital mutilation: female genital mutilation is an extremely harmful practice, and responding to it is a professional duty, not a matter of personal choice
- accessible and sensitive services: Interventions must be underpinned by accessible, high-quality, and sensitive health, education, police, social care, and voluntary sector services
- community engagement: recognising that female genital mutilation is often an embedded social norm, engagement with families and communities is essential for contributing to its eradication
- evidence-based assessments: all decisions and plans must be based on high-quality assessments, as mandated by Working Together to Safeguard Children (2023)
The Serious Crime Act (2015) significantly strengthened the existing female genital mutilation legislation by imposing a mandatory duty on healthcare professionals to report to the police any confirmed cases of female genital mutilation in females under the age of 18. This reporting must occur as soon as possible, ideally within one working day, although a maximum timeframe of one month is allowed in exceptional circumstances (HM Government, 2015b).
3 Purpose
This policy aims to provide clear guidance and a structured response to female genital mutilation, assisting all colleagues in the prevention and detection of this harmful practice. It is essential to note that the term “female” in this document refers to individuals born with a vagina, clitoris, cervix, and ovaries, representing biological sex and not gender identity.
Specifically, this guidance will support colleagues to:
- ensure early identification and safeguarding: facilitate the early identification of female genital mutilation and address any safeguarding issues for both adults and children
- appropriate information sharing and recording: establish protocols for the appropriate sharing and recording of female genital mutilation-related information
- practical guidance and support: provide practical guidance on the appropriate response and support for adults and children who have experienced or are at risk of female genital mutilation
- mandatory reporting to the police: ensure compliance with the legal requirement to report to the police if informed by a child under 18 that an act of female genital mutilation has taken place, or if physical signs of female genital mutilation are observed in a child under 18
4 Scope
This policy is applicable to all trust colleagues, agency colleagues, and other individuals, such as volunteers, who may come into contact with or receive information about safeguarding children’s issues during their duties.
For further information about responsibilities, accountabilities and duties of all employees, please see appendix A.
5 Procedure
5.1 Quick guide
5.1.1 Key point 1
Have you discussed female genital mutilation with the patient and their family? Use the quick guide for health professionals for advice with starting the conversation. Language barriers should not impede discussions about female genital mutilation; therefore, trust approved interpreter services should be used, and family members should not be employed as interpreters.
5.1.2 Key point 2
Have you completed a female genital mutilation risk assessment template and recorded your actions and the outcome of the assessment on the female genital mutilation template on the patient’s healthcare records? Ensure any risk is documented on both adults and child’s electronic record and place alert on child’s record if considered, at risk of, or undergone female genital mutilation.
5.1.3 Key point 3
If you have identified a child at risk and undergone female genital mutilation have you followed local safeguarding procedure and made a referral to children social care? Complete a safeguarding incident form to inform trust Safeguarding team.
5.1.4 Key point 4
Have you reported a known case of female genital mutilation to a child under 18 to the police under the female genital mutilation mandatory reporting duty? And shared relevant information with health professionals including GP, health visitor, school nurse and the trust Safeguarding team.
5.1.5 Key point 5
Have you considered any ongoing specialist support for anyone affected by or undergone female genital mutilation?
5.2 General health care management principles
Healthcare professionals must be aware of the countries where female genital mutilation is prevalent, and the various risk factors associated with the practice. This knowledge is essential for identifying potential cases and informing appropriate actions. The female genital mutilation safeguarding and risk assessment quick guide for health colleagues (Department of Health, 2017) provides valuable information to support these efforts.
It is crucial to be alert to indicators that female genital mutilation has already occurred, ensuring that affected individuals receive the necessary care and support. This awareness also facilitates inquiries about other female children who may require safeguarding and ensures that mandatory reporting and investigations are initiated when appropriate. The World Health Organisation (WHO, 2008) provides a formal classification of female genital mutilation, outlining four distinct types. However, it is essential to note that a physical examination is not required to confirm findings following a disclosure of female genital mutilation.
While there is no mandatory requirement to routinely ask every child and adult about their experience with female genital mutilation, healthcare professionals must be aware of the indicators and risk factors, including the patient’s country of origin. Professional judgment should be exercised to determine when it is appropriate to inquire about female genital mutilation (Department of Health, 2017).
5.3 The law in England and Wales: legal framework and obligations
The practice of female genital mutilation (FGM) is explicitly illegal within England and Wales, as established by the Female Genital Mutilation Act (2003). This legislation was significantly strengthened by the Serious Crime Act (2015), which introduced mandatory reporting requirements for specified professionals. Specifically, healthcare colleagues are now legally obligated to report to the police any known cases of female genital mutilation identified in females under the age of 18 during the course of their professional duties.
Furthermore, the Serious Crime Act (2015) introduced the use of female genital mutilation protection orders (FGMPOs), which are civil orders designed to protect children at risk of female genital mutilation and to provide lifelong anonymity for victims. These orders empower the courts to take proactive measures to prevent female genital mutilation and to safeguard those who have already experienced it.
Additional offences introduced by the Serious Crime Act (2015) include:
- extra-territorial jurisdiction: this provision allows for the prosecution of UK nationals who commit female genital mutilation abroad, ensuring that individuals cannot evade legal consequences of performing female genital mutilation outside the UK
- offence of failing to protect a child: this offence holds individuals accountable for failing to take reasonable steps to protect a child from the risk of female genital mutilation
For a more comprehensive understanding of the legal framework, healthcare professionals should refer to chapter 3 of the multi-agency statutory guidance on female genital mutilation (HM Government, 2020).
5.4 Female genital mutilation mandatory reporting: legal duty and compliance
The mandatory reporting duty for female genital mutilation is a legal obligation, as stipulated in the Female Genital Mutilation Act (2003) amended by the Serious Crime Act (2015). Failure to comply with this duty is likely to result in disciplinary measures, which may include referral to the relevant professional regulator.
The legislation mandates that regulated health professionals in England must report to the police when, during their professional duties, they:
- are informed by a female child or young person under the age of 18 that an act of female genital mutilation has been carried out on them
- observe physical signs that appear to indicate an act of female genital mutilation has been carried out on a female child or young person under the age of 18, and they have no reason to believe that the act was necessary for the child’s physical or mental health, or for purposes connected with labour or birth
Reports under this duty should be made as soon as possible, with best practice dictating that this should occur by the end of the next working day. However, to accommodate exceptional circumstances, a maximum timeframe of one month is permitted.
For the purpose of mandatory reporting, the age of the female is defined as any female currently under the age of 18. This means that the duty does not apply when a woman aged 18 or over discloses that she had female genital mutilation when she was under 18.
Compliance with the mandatory reporting duty does not breach any confidentiality requirements or other restrictions on disclosure that might otherwise apply. The duty is a personal duty, meaning that the individual professional who becomes aware of the case is responsible for making the report; this responsibility cannot be transferred. The only exception to this is if the professional is aware that another individual from their profession has already made a report, in which case there is no requirement to make a second report.
5.5 Female genital mutilation protection orders (FGMPO): civil protection measures
A female genital mutilation protection order (FGMPO) is a civil order that may be issued for the purpose of protecting a child who is at risk of female genital mutilation, or against whom a female genital mutilation offence has been committed. The court has the authority to make an order that prohibits, requires, or restricts actions as it deems appropriate to prevent individuals from subjecting a child to female genital mutilation, or from arranging or committing female genital mutilation.
Examples of the types of orders the court might make include:
- protecting a victim or potential victim from being taken abroad to undergo female genital mutilation
- ordering the surrender of passports or any other travel documentation of the child to be protected
- including terms that relate to the conduct of individuals named in the order, both inside and outside of England and Wales
It is important to note that orders may be made against individuals who are not explicitly named in the application, recognising that multiple individuals within the wider community may be involved in female genital mutilation-related activities.
5.6 Safeguarding principles: adults, ensuring support and respect
When an adult patient discloses that they have undergone female genital mutilation, or if a healthcare professional suspects that an adult has undergone female genital mutilation or is at risk of female genital mutilation, it is essential to consider the physical and emotional needs of the woman. Consent should be obtained before signposting or referring the woman to appropriate specialist services.
When discussing female genital mutilation with a woman, it is crucial to ensure that she is seen alone and that the discussion is conducted with sensitivity, recognising the intimate nature of the subject. Language barriers should not impede discussions about female genital mutilation; therefore, trust-approved interpreter services should be used, and family members should not be employed as interpreters.
If the woman is pregnant or has female children, the welfare of the unborn child and other female members of her extended family must also be considered. Risk assessment tools provided by the Department of Health (2017) can be used to support healthcare professionals in evaluating the safeguarding risks posed to both girls and women. These assessments should include consideration of the woman’s country of origin, presenting clinical symptoms, and other relevant social information.
While there is no mandatory requirement for the automatic referral of adult women to social care or the police, as there is with children, support should be offered if the woman wishes to report female genital mutilation as a crime.
If the adult patient is considered vulnerable or at risk, local safeguarding procedures should be followed.
5.7 Additional safeguarding considerations: addressing related issues
5.7.1 Domestic abuse
Female genital mutilation and forced marriage, which may accompany female genital mutilation, are recognised as forms of domestic abuse where the alleged perpetrator has a personal connection to the victim. Healthcare professionals should be vigilant in identifying and addressing any other acts of controlling or coercive behaviour. Local safeguarding procedures should be followed, and the trust’s domestic abuse policy should be consulted for further guidance.
5.7.2 Breast flattening
In some countries, breast flattening or ironing, which involves the use of heated stones, hammers, or spatulas to compress breast tissue, is practiced. This practice is performed to disguise the onset of puberty in females, with the belief that it will deter male attention and protect them from sexual harassment, assault, exploitation, and rape or sexually transmitted diseases.
Although there is no specific law within the UK regarding breast flattening or ironing, it is considered a form of physical abuse. If healthcare professionals are concerned that a child may be at risk of, or suffering significant harm from, this practice, they must refer to their local safeguarding procedures.
It should also be acknowledged that some young people may choose to bind their breasts using constrictive material due to gender transformation or identity. This must be taken into account when assessing a young person.
5.8 Safeguarding principles: children, protecting the vulnerable
Female genital mutilation is a harmful and illegal act to which a child is unable to resist or consent. Female genital mutilation places a child at risk of, or causes them to suffer, significant harm, as defined under section 47 of the Children Act (1989), and is classified as a form of physical child abuse. Therefore, it must be addressed within the framework of child protection, as outlined in Working Together to Safeguard Children (2023).
Language barriers should not impede discussions about female genital mutilation; therefore, trust approved interpreter services should be used, and family members should not be employed as interpreters.
When female genital mutilation is suspected in a child, or there is a risk that it may take place, healthcare professionals should:
- contact the police immediately if they suspect that a child is at immediate risk of harm from female genital mutilation
- make a referral to children’s social care in accordance with local safeguarding children’s board procedures
- inform their line manager and the trust Safeguarding team for advice
- if a child has undergone female genital mutilation, report the case to the police as a mandatory duty
- share information with the child’s GP, health visitor, or school nurse.
- complete the female genital mutilation data set on the child’s SystmOne records, which can be found in the safeguarding templates
- complete an incident reporting form
Given that cases involving female genital mutilation can be complex and dependent on various factors and circumstances, the management of each case must be assessed on an individual basis. Advice and guidance can be accessed from:
- Rotherham, Doncaster and South Humber NHS Foundation Trust named doctor safeguarding children
- Rotherham, Doncaster and South Humber NHS Foundation Trust nurse consultant safeguarding
- Rotherham, Doncaster and South Humber NHS Foundation Trust named nurse or professional safeguarding children and adults.
- children or adult social care
- the police
- the National Society for the Prevention of Cruelty to Children (NSPCC)
5.9 Documentation and data collection: enhancing safeguarding efforts
The Department of Health’s female genital mutilation prevention program is supported by:
- delivering a digital system to strengthen the safeguarding of girls at risk of female genital mutilation. This system, known as the female genital mutilation information sharing (FGM-IS) system, provides a national information technology infrastructure for healthcare professionals to record that a girl has a family history of female genital mutilation. The FGM-IS is integrated into the NHS Spine. The Safeguarding team can view, add, and remove the female genital mutilation indicator, which can be accessed via the summary care record application (SCRa) or through local clinical systems integrated with FGM-IS
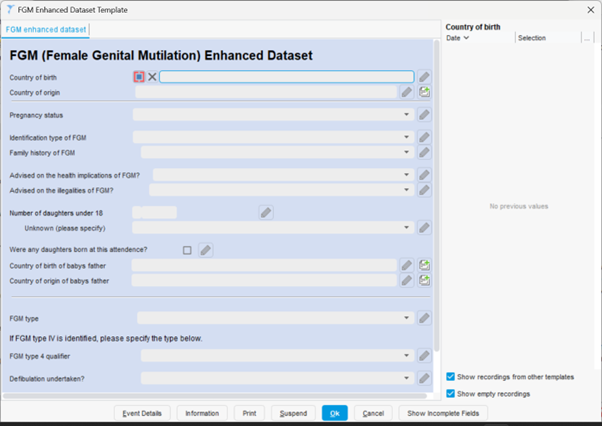
- presenting a national picture of the prevalence of female genital mutilation across the NHS in England. This is achieved through the female genital mutilation enhanced dataset. NHS Digital collects data on female genital mutilation within the NHS in England on behalf of the Department of Health (DH). The data collected is used to produce information that helps to:
- improve how the NHS supports women and girls who have had or who are at risk of female genital mutilation
- plan local NHS services to address current and future needs
- help other organisations, such as local authorities, develop plans to prevent female genital mutilation in local communities
Data is collected from NHS acute trusts, mental health trusts, and GP practices, and reports are published as official statistics every quarter.
If female genital mutilation is disclosed or identified during a healthcare consultation, this should be documented within the female genital mutilation page in the patient’s electronic records. This can be accessed within the safeguarding template.
Under “female genital mutilation” row.
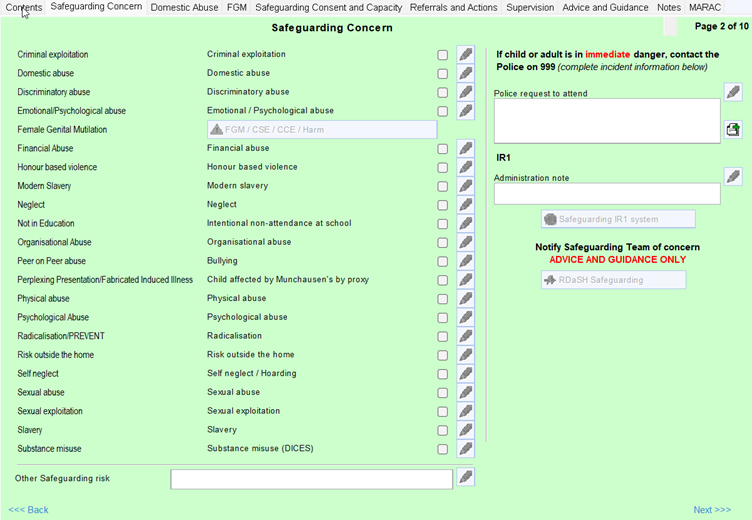
Then “female genital mutilation enhanced dataset template” under “family history of female genital mutilation”.
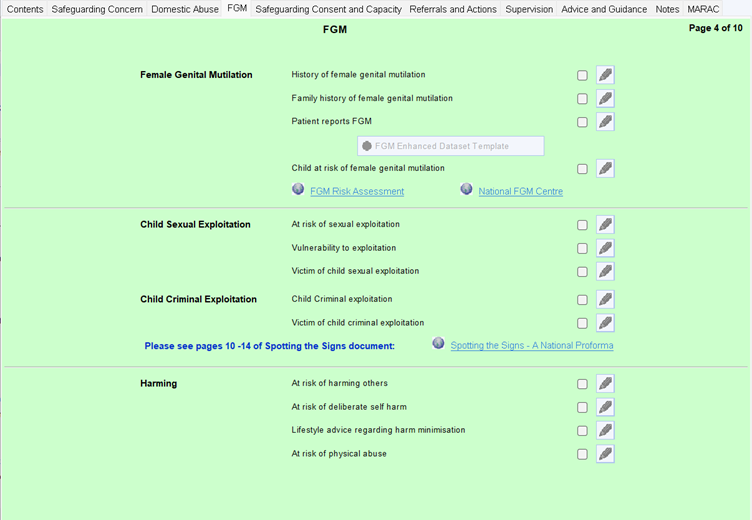
Documentation should include:
- completion of the female genital mutilation template, for example, female genital mutilation identified, parent has undergone female genital mutilation, child at risk of female genital mutilation including the female genital mutilation enhanced dataset within the safeguarding template
- all observations made relating to the identification of female genital mutilation or risk of female genital mutilation
- all actions taken
- all information shared and with whom or, documentation why they have chosen not to share information
- alert added to front page of patients records
Please note if during a consultation with an adult female you have identified a child at risk, this must be recorded in both the adult and child’s records using the female genital mutilation page within the safeguarding module.
An incident reporting form should then be completed for every case of female genital mutilation that is identified ensuring the incident is recorded as child or adult safeguarding, even if this has not subsequently resulted in a referral to social care. This reporting mechanism is to ensure that the Safeguarding team have oversight of all cases involving female genital mutilation.
5.10 Information sharing
In the UK, the duty to share information where there is a concern or risk to a person or child’s welfare, is more important than the right to confidentiality. Healthcare colleagues have a professional and statutory duty to record, refer and share information where there is a significant public interest to do so. Information sharing is a crucial part of early intervention and prevention of female genital mutilation.
If identified by a healthcare professional, information should be shared with the child’s GP, health visitor or school nurse (dependent on age of child) and potentially other professional delivering care to the child depending upon circumstances.
Where colleagues remain in doubt regarding information sharing, they should contact the trust Safeguarding team for advice.
If a decision is taken not to share, then the reason for this should be documented clearly in the patients’ healthcare record.
6 Training implications
6.1 Recognising and preventing female genital mutilation
6.1.1 All colleagues required to undertake level 3 safeguarding adults and children training
- How often should this be undertaken: once.
- Length of training: 60 minutes.
- Delivery method: e-learning
- Training delivered by whom: government training.
- Where are the records of attendance held: electronic staff record (ESR).
8 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
8.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
As a consequence the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
8.1.1 How this will be met
No issues have been identified in relation to this policy.
8.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
8.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005).
9 Links to any other associated documents
- Domestic abuse policy
- Female genital mutilation classification
- Female genital mutilation protection orders guidance
- Female genital resource pack
- Female genital mutilation safeguarding and risk assessment quick guide for health colleagues
- Female genital mutilation safeguarding pathway
- Multiagency statutory guidance on female genital mutilation
- National female genital mutilation centres: resources for health
- Safeguarding adults policy
- Safeguarding children policy
10 References
- Children Act (1989) Children Act (1989)
- Department for Education (2023) Working Together to Safeguard Children
- Department of Health (2017) Female genital mutilation safeguarding and risk assessment quick guide for health professionals
- HM Government (2020) Multi-agency statutory guidance on female genital mutilation
- Legislation (2019) Female Genital Mutilation Act (2003)
- NHS Digital Female Genital Mutilation Datasets
- The National Society for the Prevention of Cruelty to Children (NSPCC) (2023) The National Society for the Prevention of Cruelty to Children helpline
- UK Government (2015) Serious Crime Act (2015)
- UNICEF (2022) United Nations convention on the rights of the child (UNCRC)
11 Appendices
11.1 Appendix A responsibilities, accountabilities and duties
The trust, the chief executive and directors of the trust are responsible for ensuring that robust systems are in place to identify and manage the risks associated with safeguarding adult and children at risk and to support the effective multiagency partnership working and responses which are required.
This includes the identification and training of suitable colleagues to fulfil the roles set out within the multiagency safeguarding procedures. All colleagues are responsible for fulfilling their responsibilities to safeguard adults and children at risk.
The trust’s nominated executive director: the trust has a nominated executive director for safeguarding, who takes a professional lead in promoting best practice in safeguarding at board level. In this trust, the nominated executive director for safeguarding is the director of nursing and allied health professionals.
Deputy chief nurse (operational lead) has responsibility to provide expert advice, strategic and operational leadership for safeguarding and professional standards. To continually develop a proactive approach to safeguarding through collaboration with the local authority and other agencies. To ensure all mandatory and statutory requirements around safeguarding are met and develop support systems.
The head of safeguarding has responsibility to provide expert advice, strategic and operational leadership for safeguarding and professional standards. To continually develop a proactive approach to safeguarding through collaboration with the local authority and other agencies. To ensure all mandatory and statutory requirements around safeguarding are met and develop support systems.
Named nurses or named professionals (practice leads) have responsibility to provide an expert professional leadership role in relation to safeguarding. To work at a strategic level across the health and the social care community, fostering and facilitating multiagency working and training in respect of safeguarding. To act as an expert resource on safeguarding issues, providing accessible, accurate and relevant information to colleagues.
The named nurses or professionals are responsible for delivering support, advice and guidance to the safeguarding managers, safeguarding supervisors and enquirers.
They have a key role in promoting best practice and are available as a source of advice or guidance and support for managers and colleagues involved in safeguarding.
Service managers, modern matrons or area clinical managers are responsible for:
- ensuring all colleagues have access to the relevant multiagency safeguarding procedures in their workplace
- maintaining compliance with the policy and multiagency safeguarding procedures within their services
- arranging colleagues attendance at training, updates in relation to safeguarding
- providing support for colleagues involved in safeguarding
Employees of the trust: safeguarding is everybody’s business.
All employees (including volunteers) have a responsibility to safeguard and promote the wellbeing of children and adults at risk of harm. Employees must be able to recognise and report safeguarding concerns to their line manager or the Safeguarding team to ensure actions can be taken to address the concerns.
11.2 Appendix B monitoring arrangements
11.2.1 Adherence to safeguarding procedures
- How: monitoring of incident reporting and national reporting system.
- Who by: Safeguarding team.
- Reported to: safeguarding and mental capacity assurance group.
- Frequency: annually and as reporting of incidents occur.
11.3 Appendix C actions to be taken if a child or young person is at risk of female genital mutilation
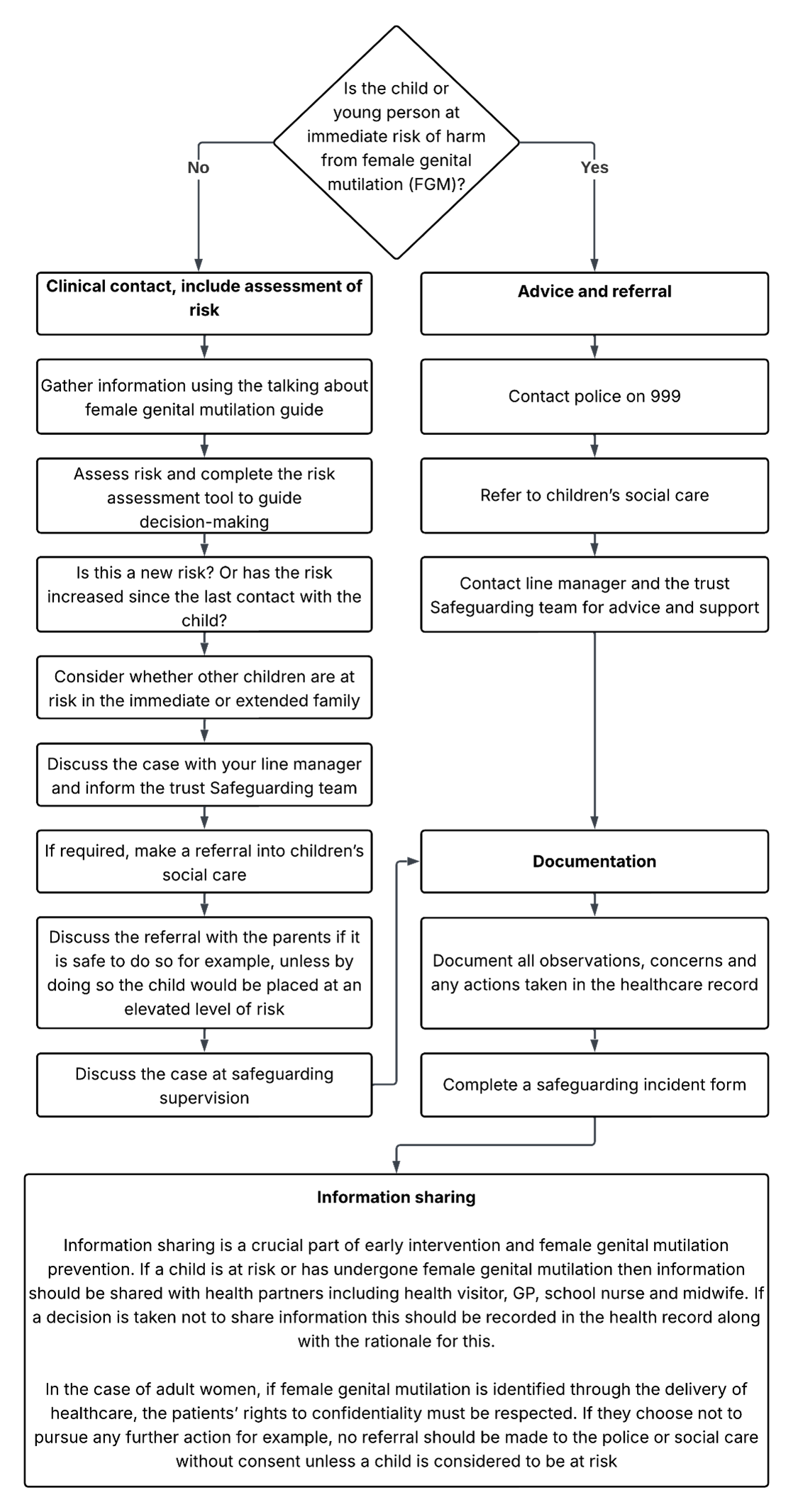
11.3.1 Child or young person at immediate risk of harm from female genital mutilation
- Contact police on 999.
- Refer to children’s social care.
- Contact line manager and the trust Safeguarding team for advice and support.
11.3.2 Child or young person is not at immediate risk of harm from female genital mutilation
- Clinical contact, include assessment of risk.
- Gather information using the talking about female genital mutilation guide.
- Assess risk and complete the risk assessment tool to guide decision-making.
- Is this a new risk? Or has the risk increased since the last contact with the child?
- Consider whether other children are at risk in the immediate or extended family.
- Discuss the case with your line manager and inform the trust Safeguarding team.
- If required, make a referral into children’s social care.
- Discuss the referral with the parents if it is safe to do so for example, unless by doing so the child would be placed at an elevated level of risk.
- Discuss the case at safeguarding supervision.
11.3.3 Documentation
- Document all observations, concerns and any actions taken in the healthcare record.
- Complete a safeguarding incident form.
11.3.4 Information sharing
- Information sharing is a crucial part of early intervention and female genital mutilation prevention. Consider sharing information with: health visitor, GP, school nurse and midwife.
- If a decision is taken not to share information this should be recorded in the health records with the rationale for this.
11.4 Appendix D actions to be taken if someone has already been subjected to female genital mutilation
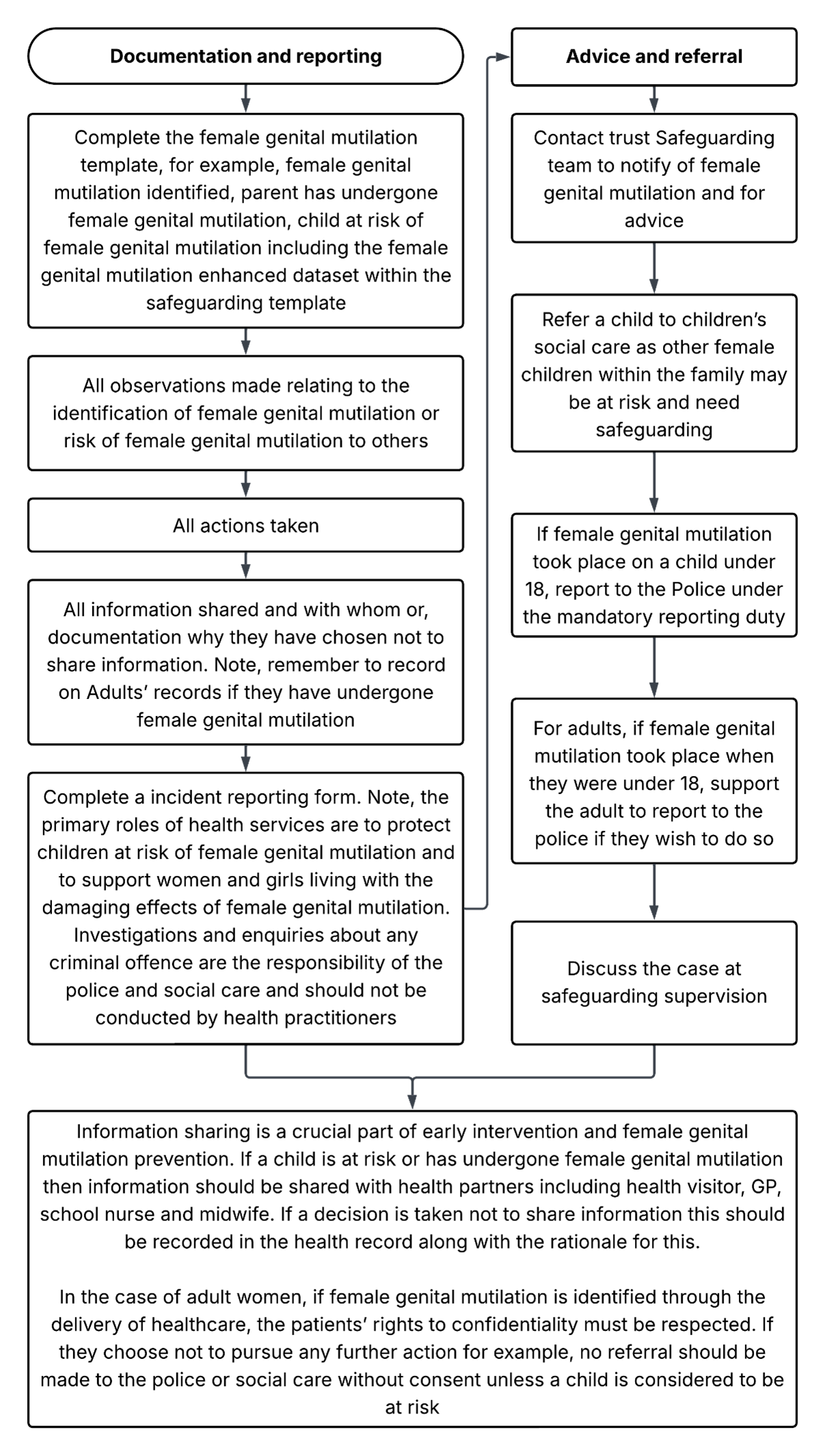
11.4.1 Documentation and reporting
- Complete the female genital mutilation template, for example, female genital mutilation identified, parent has undergone female genital mutilation, child at risk of female genital mutilation including the female genital mutilation enhanced dataset within the safeguarding template.
- All observations made relating to the identification of female genital mutilation or risk of female genital mutilation to others.
- All actions taken.
- All information shared and with whom or, documentation why they have chosen not to share information. Note, remember to record on Adults’ records if they have undergone female genital mutilation.
- Complete an incident reporting form. Note, the primary roles of health services are to protect children at risk of female genital mutilation and to support women and girls living with the damaging effects of female genital mutilation. Investigations and enquiries about any criminal offence are the responsibility of the police and social care and should not be conducted by health practitioners.
11.4.2 Advice and referral
- Contact trust Safeguarding team to notify of female genital mutilation and for advice.
- Refer a child to children’s social care as other female children within the family may be at risk and need safeguarding.
- If female genital mutilation took place on a child under 18, report to the Police under the mandatory reporting duty.
- For adults, if female genital mutilation took place when they were under 18, support the adult to report to the police if they wish to do so.
- Discuss the case at safeguarding supervision.
11.4.3 Information sharing
Information sharing is a crucial part of early intervention and female genital mutilation prevention. If a child is at risk or has undergone female genital mutilation then information should be shared with health partners including health visitor, GP, school nurse and midwife. If a decision is taken not to share information this should be recorded in the health record along with the rationale for this.
In the case of adult women, if female genital mutilation is identified through the delivery of healthcare, the patients’ rights to confidentiality must be respected. If they choose not to pursue any further action for example, no referral should be made to the police or social care without consent unless a child is considered to be at risk
Document control
- Version: 2.
- Unique reference number: 1045.
- Approved by: clinical policies review and approval group.
- Date approved: 1 July 2025.
- Name of originator or author: nurse consultant for safeguarding.
- Name of responsible individual: chief nursing officer.
- Date issued: 29 July 2025.
- Review date: 31 July 2028.
- Target audience: all colleagues within the trust.
Page last reviewed: August 20, 2025
Next review due: August 20, 2026
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem