1 Policy summary
NHS services specifically commissioned mental health, learning disability and autism services, and local authorities have a statutory duty to cooperate with multi-agency public protection arrangements (MAPPA). All colleagues working with patients and carers should understand which patients are eligible for management under multi-agency public protection arrangements, and, as necessary, identify, notify and refer such patients, contributing to multiagency risk management plans.
The trust has a multi-agency public protection arrangement lead who provides a single point of contact for case-related matters and multi-agency public protection arrangements representatives in Rotherham, Doncaster and South Humberside.
All multi-agency public protection arrangement eligible patients will be identified within the clinical records system and when appropriate they will be notified or referred to the multi-agency public protection arrangements coordinator. Information will be shared with multi-agency public protection arrangements agencies when it is lawful, necessary and proportionate to do so. For patients being managed at level 2 or 3, the clinical team delivering the current will contribute to the development of multi-agency risk management plans.
2 Introduction
Multi-agency public protection arrangements (MAPPA) is a framework of statutory arrangements introduced by the Criminal Justice Act (CJA) 2003, through which the police, probation and prison services (jointly comprising the multi-agency public protection arrangements responsible authority) work together with other agencies to manage the risks posed by violent and sexual offenders, in order that re-offending is reduced and the public are protected. Multi-agency public protection arrangements is not a statutory body but is a mechanism through which agencies can better discharge their statutory responsibilities and protect the public in a coordinated way. Agencies at all times retain their full statutory responsibilities and obligations.
Under section 325(3) of the Criminal Justice Act (2003) certain agencies have a “duty to co-operate” with the Responsible Authority, for the purpose of assessing and managing the risks posed by multi-agency public protection arrangement offenders. Health organisations are among those organisations with a statutory duty to cooperate with multi-agency public protection arrangements and mental health trusts are among those organisations with a responsibility to identify patients who are multi-agency public protection arrangement eligible.
The policy should be considered in conjunction with the care programme approach (CPA), clinical risk assessment and management policies of the trust, alongside the domestic abuse, child and adult safeguarding policies.
3 Purpose
- To ensure Rotherham, Doncaster and South Humber NHS Foundation Trust (RDaSH) colleagues understand their legal and clinical responsibilities under multi-agency public protection arrangements (MAPPA).
- To support effective risk management of individuals who pose a serious risk to the public.
- To promote safe discharge planning, community integration, and safeguarding.
4 Scope
- Patients who meet multi-agency public protection arrangements (MAPPA) criteria (for example, violent or sexual offenders).
- Mental health professionals involved in risk assessment and care planning.
- NHS trusts with statutory duties to cooperate under the Criminal Justice Act (2003).
The duty to cooperate with multi-agency public protection arrangements is an obligation for the trust as an organisation, rather than for mental health professionals as individuals. All colleagues working with patients and carers need to be aware of this policy to know how and when it might impact on their practice, and to understand how conflicts between the organisation’s statutory obligations and an individual’s professional obligations should be resolved.
Considering whether to share information is particularly important when an offender is to move out of a supervised or contained environment into a community setting. This may include unescorted leave of absence under section 17 of the Mental Health Act (1983), discharge from inpatient status and release from prison.
Very few of the patients receiving care from the trust will, at any one time, come within the multi-agency public protection arrangements (MAPPA) definition of a violent or sexual offender and thereby be eligible for management under multi-agency public protection arrangements. Occasionally, there will be patients who pose a very serious risk of harm, but who are not violent or sexual offenders for multi-agency public protection arrangement purposes. While management of these latter cases may not be within the formal multi-agency public protection arrangements framework, cases should be discussed with the multi-agency public protection arrangements representative for the locality.
The role of NHS trusts is outlined in chapter 26 of the statutory multi-agency public protection arrangements guidance, which was updated in 2022 and can be found on the national multi-agency public protection arrangements website.
5 Procedure
5.1 Inpatient admission
The responsible clinician should be aware of or identify whether the patient meets category 1 or category 2 of the multi-agency public protection arrangements (MAPPA) guidance (appendix A) and the level of management (appendix B) and record this in the electronic patient record.
If the responsible clinician is unable to determine whether the patient is a category 1 or category 2 multi-agency public protection arrangements, they should contact the Multi-Agency Public Protection Arrangements Unit to establish the category and discuss with the multi-agency public protection arrangements representative.
For South Yorkshire the Multi-Agency Public Protection Arrangements Unit can be contacted on 0114 252 3377.
For Humberside, email yathps.northeastlincolnshire.mappa@justice.gov.uk.
A multi-agency public protection arrangement (MAPPA) I form should also be completed on admission by the responsible clinician if admitted under the Mental Health Act.
If category 1 they will be on the sex offenders register and information regarding transfer to the service should already have been handed over to the police before admission from where they have transferred from. However, this should not be assumed
The local police Violent and Sex Offender Register (ViSOR) Unit needs to be aware of any category 1 registered sex offender (RSO) patients detained locally so it should be contacted as soon as possible by colleagues (this includes registered sex offenders transferred from other hospitals)
The police will want to visit the patient to explain the notification requirements relating to their eventual release into the community.
If, on the other hand, the patient was a registered sex offender already living in the community who has been detained for another reason, then the patient is responsible for informing the police of their change of residence within 3 days. Hospital colleagues should ensure this happens. Please note that the Violent and Sex Offender Register is updated on completion of the multi-agency public protection arrangements (MAPPA) I form.
Note, there may be patients who lack the capacity to understand their status on the sex offenders’ register or the registering requirements and, in these cases, would benefit from a best interest decision made by the responsible clinician, under the Mental Capacity Act to do this on their behalf.
5.2 During admission
5.2.1 Category 1
During treatment with the service the police will need to follow the requirements of the sex offenders register during the patient’s stay. This may involve them visiting or attending meetings.
5.2.2 Categories 1, 2 and 3
The Violent and Sex Offender Register (ViSOR) Unit and, or probation service (if involved) must be kept informed:
- if a serious incident occurs whilst they are an inpatient
- if the patient requires emergency treatment in an acute hospital
The Multi-Agency Public Protection Arrangements Unit must be kept informed:
- when the patient is being considered for leave (escorted or unescorted)
- when the patient is being considered for discharge
5.3 Prior to granting section 17 leave for category 1 or 2, or potential category 3, that is high risk of serious harm offenders detained as notional section 37s) multi-agency public protection arrangements patients
The multi-agency public protection arrangements (MAPPA) I notification form (see relevant documents) should be completed prior to any decision by the responsible clinician (RC) to grant section 17 Leave and the form sent to the multi-agency public protection arrangements representative and the trust Safeguarding team rdash.safeguardingadults@nhs.net.
The form should be received back from the multi-agency public protection arrangement representative to allow sharing of pertinent information regarding risks associated with the patient, prior to any leave being granted.
The multi-agency public protection arrangement representative will share this information with the Violent and Sex Offender Register (ViSOR) Unit who will liaise directly with the responsible clinician over any potential risks in relation to the leave and any future notification requirements that they will require.
The responsible clinician should also be mindful of any responsibilities under the Victim Contact (VC) Scheme, especially regarding leave (escorted or unescorted) for section 37 and 41 patients and liaise with the Victim Contact Unit accordingly, if it is involved.
5.4 Prior to discharge planning
During discharge planning, the multi-agency public protection arrangements or Violent and Sex Offender Register (ViSOR) Unit may, on a case-by-case basis, be more involved in terms of meetings and agreeing discharge plans.
The responsible clinician also needs to be mindful of any responsibilities under the Victim Contact Scheme, liaising with the Victim Contact Unit or directly with any relevant victim if appropriate.
Unless the patient is to be under the supervision of the probation service (on prison licence) on discharge (in which case probation will be the lead agency), it is the responsibility of the responsible clinician to decide, prior to any discharge planning and having consulted with the Multi-Agency Public Protection Arrangements Unit, police, the Victim Contact Unit (if involved), and any other relevant agencies, whether a referral is needed to the Multi-Agency Public Protection Arrangements Unit for management at multi-agency public protection arrangements level 2 or 3 (full multidisciplinary team (MDT) oversight), or whether, in their view, the case can be managed at level 1 (under care programme approach in the clinical mental health team) in the community.
The exact timing of notification is a matter for the multidisciplinary team to consider. This consideration should begin as soon as a patient has been identified as multi-agency public protection arrangements eligible.
The team should take into account the level of risk associated with the case, the guiding principles around confidentiality, the likely time period until the patient will have community access, the possibility of the patient gaining access to the community precipitously and the importance of ensuring that notification occurs reliably.
Note, the probation service will be the lead agency for offenders detained during a prison sentence of 12 months or more, by section 45A direction or section 47 or section 49 transfer and discharged prior to the sentence expiry date (SED).
The multi-agency public protection arrangements level, once decided, prior to discharge, should be recorded on the electronic patient health record using the multi-agency public protection arrangements template.
5.5 Community services
For existing patients’ care co-ordinators should be aware of which patients are multi-agency public protection arrangements (MAPPA) eligible and should be managing these patients under the multi-agency public protection arrangements policy.
If colleagues believe that the patient is multi-agency public protection arrangement eligible, then contact with the Multi-Agency Public Protection Arrangements Unit should be made, to establish the facts and determine the category and level and they should then ensure this is recorded on the electronic patient health record using the multi-agency public protection arrangements template.
5.5.1 On receipt of a referral to the trust
For any new patients referred to the service care co-ordinator should be aware of or identify whether the patient is a multi-agency public protection arrangements (MAPPA) offender and:
- what multi-agency public protection arrangements category they are
- who the lead agency is, if not mental health or learning disability services
- what multi-agency public protection arrangements level they are being managed at
Colleagues should determine whether they meet category 1, 2 or 3 of the multi-agency public protection arrangements guidance (appendix A) and are managed at level 1, 2 or 3 (appendix B).
If colleagues are unable to determine whether the patient is a category 1, 2 or 3 multi-agency public protection arrangements, they should contact the multi-agency public protection arrangements Unit to establish the category and level and discuss with the multi-agency public protection arrangements representative.
For any patients who are made subject to a conditional discharge under the Mental Health Act 1983 (section 37 or section 41), or a community treatment order receded by a section 37 or a notional section 37, colleagues should have been made aware of whether they are category 1, 2 or 3 and what multi-agency public protection arrangements level they are to be managed at, by the discharging hospital.
If category 1 they will be on the sex offenders register and information regarding transfer to our service should already have been handed over to the Police from where they have transferred from. However, this should not be assumed. The patient has 3 days to re-register with the local Police Violent and Sex Offender Register (ViSOR) Unit, and it is their responsibility to do so.
Note, there may be patients who lack the capacity to understand their status on the sex offenders register or the registering requirements and, in these cases, we should ensure, under the Mental Capacity Act a best interest decision is made and that we do this on their behalf.
5.6 Ongoing care with trust services
Colleagues must ensure that the patients are managed in accordance with the multi-agency public protection arrangements policy.
5.7 Recording of multi-agency public protection arrangements offenders onto the trust’s electronic patient recording system by the multi-agency public protection arrangements representatives
Within the trust there are 3 local trust multi-agency public protection arrangements representatives:
5.7.1 Multi-agency public protection arrangements representatives
-
Rotherham
-
North Lincolnshire
5.7.2 Multi-agency public protection arrangements lead
The trust multi-agency public protection arrangements lead is the Head of Safeguarding Louise Bertman: louise.bertman@nhs.net.
5.7.2 Multi-agency public protection arrangements coordinators
-
South Yorkshire
-
North Lincolnshire
For those patients that are known to the trust and have a record on the electronic patient recording system the trust multi-agency public protection arrangements representatives who attend the multi-agency public protection arrangements level 2 meetings have the responsibility for ensuring that the appropriate care co-ordinator is invited to attend the multi-agency public protection arrangements meeting with them.
Following attendance at the multi-agency public protection arrangements meeting, the trust multi-agency public protection arrangements representatives will ensure that:
- an alert is created on the electronic patient record
- the multi-agency public protection arrangements template in the electronic patient record needs completing
- see appendix D
- an email is sent to the appropriate care coordinator or team manager to advise them of the alert
- an email is sent to the trust Safeguarding team
5.8 Change of address of multi-agency public protection arrangements patients
For any patients who are subject to multi-agency public protection arrangements (MAPPA) and who change their address whilst in the care of the trust this information must be notified to the Multi-Agency Public Protection Arrangements Unit. It is the responsibility of the multi-agency public protection arrangements representative to ensure that the social supervisor (a social supervisor is an appropriately qualified mental health professional who has a responsibility to report to the Secretary of State on a conditionally discharged restricted patient’s progress in the community) completes the notification of change of address form (see relevant documents) and forward this to the appropriate multi-agency public protection arrangements co-ordinator:
-
Rotherham and Doncaster
5.9 Third party disclosure
In order to protect the public from serious harm, there are occasions where information needs to be disclosed to another person (member of the public or non-multi-agency public protection arrangements agency) in order to either protect them directly from the offender, or for them to protect others. For example, leisure centre staff might be alerted where a local offender is felt to pose a risk to those using the centre. This could also involve accommodation providers, new partners, employers and churches. The need for this should be kept under review at all times, it would be a shared care team decision rather than an individual team members decision to disclose information, and it applies to all multi-agency public protection arrangements offenders whatever the category or level.
When information is disclosed, it will always be to ensure that the public is being protected and will be the minimum necessary to manage the risk. The person disclosing the information will explain why the information is being disclosed and give advice on what will happen afterwards.
The offender should also be consulted beforehand (unless this would be counter-productive). They should be told what information will be disclosed on the notification form, and under what circumstances additional information would be shared. Whether or not the patient consents to such information sharing should be recorded within the clinical records.
If the patient does not consent, the care team should consider whether to breach confidentiality in the public interest. If the team decides that it is not appropriate to breach confidentiality or there is an irresolvable difference of opinion within the team, then the case should be discussed with the trust multi-agency public protection arrangements lead.
In circumstances where social supervisors feel that there is information which needs to be disclosed, they should first consult the National Guidance (2024) Chapter 10 on disclosure and discuss this with their team manager and any other agencies involved (especially the police and the lead agency) via a clinical multi-disciplinary team meeting, inviting the trust’s information governance manager.
Careful thought needs to be given to such things as:
- should a level 2 meeting be convened first?
- who is the lead agency and what is their view?
- who “owns” the information?
- who should do the disclosure?
- exactly what should be disclosed?
If it is felt that disclosure is warranted, they should complete the application for third party disclosure form (see relevant documents) and the trust’s information governance manager will review and report back to the social supervisor. The trust multi-agency public protection arrangements lead should also be informed.
5.10 Exit from multi-agency public protection arrangements
For each patient subject to multi-agency public protection arrangements management, the care team should be aware of when the patient’s multi-agency public protection arrangements eligibility will end and plan for this. See appendix D.
Where the multi-agency public protection arrangements eligibility of a patient being managed at level 1 is due to expire, the care team should consider whether the case may then come within category 3 and warrant referral for active multi-agency management at level 2 or 3.
When the multi-agency public protection arrangement eligibility of a patient being managed at level 1 ends, the care team must inform the multi-agency public protection arrangements representative of this and record the patient’s exit from multi-agency public protection arrangements on the multi-agency public protection arrangements eligibility form.
5.11 Strategic oversight
The head of safeguarding is the multi-agency public protection arrangements lead for the trust, who:
- acts as a single point of contact with the responsible authority for operational matters
- has overall responsibility for this policy and monitoring practice.
- oversees the provision of information sharing to trust colleagues about updates, procedures, legislation and resources about multi-agency public protection arrangements
The multi-agency public protection arrangements representatives are a source of advice for clinical colleagues on case-related matters.
The trust Safeguarding team will facilitate the sharing of information between clinicians and multi-agency public protection arrangements representatives where required.
6 Training implications
6.1 Trust wide induction
- Employee groups requiring training: responsible clinicians and care co-ordinators.
- Frequency: once as part of trust wide induction.
- Length of training: incorporated into the trust wide induction agenda.
- Delivery method: face to face.
- Training delivered by: Daniel Kirk, multi-agency public protection arrangements representative for Rotherham.
- Where are the records of attendance held: electronic staff record (ESR).
7 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
7.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
Consequently, the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity, and respect, (when appropriate this should also include how same sex accommodation is provided).
7.1.1 How this will be met
No issues have been identified in relation to this policy.
7.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individual’s capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individuals’ informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all colleagues working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason, all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005)to ensure that the rights of individual are protected, and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
7.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005).
8 Links to any other associated documents
- Safeguarding children policy
- Safeguarding adults policy
- Domestic abuse policy
- Care programme approach (CPA) policy
- Clinical risk assessment and management policy
- Rotherham multi-agency public protection arrangements policy
- Doncaster multi-agency public protection arrangements policy
- North Lincolnshire multi-agency public protection arrangements (MAPPA) policy
- HM Prison and Probation Service guidance
- National multi-agency public protection arrangements policy
- Multi-agency public protection arrangements guidance 2012, 4th edition, part 2, Appendices and forms (staff access only)
- Identification of multi-agency public protection arrangements offenders and screen tool (staff access only)
- Initial notification of multi-agency public protection arrangements (MAPPA) I
- Change of address form
- Sharing third party information form
- Guidance for working with multi-agency public protection arrangements and mentally disordered offenders, schedule offences (staff access only)
- List of contacts for South Yorkshire (staff access only)
- Multi-agency public protection arrangements (MAPPA) A referral to multi-agency public protection arrangements level 2 or 3 (staff access only)
- List of serious further offences (staff access only)
9 References
- Birmingham and Solihull Mental Health Foundation NHS Trust (2024) multi-agency public protection arrangements
- Criminal Justice Act (2003)
- HM Prison and Probation Service (2024) multi-agency public protection arrangements guidance
- Mental Health Act (1983)
10 Appendices
10.1 Appendix A categories of multi-agency public protection arrangements eligible offenders
There are 4 categories:
10.1.1 Category 1: registered sex offenders
Any patient who is currently a registered sex offender or applies to anyone convicted of, cautioned for, found not guilty by reason of insanity of, or found unfit to plead in relation to an offence listed in schedule 3 of the Sexual Offences Act (2003)
The notification period varies according to sentence:
- indefinite if imprisonment for more than 30 months or restricted hospital order
- 10 years if imprisonment for between 6 and 30 months
- 7 years if imprisonment for less than 6 months or unrestricted hospital order
10.1.2 Category 2: violent and other sex offenders
An individual who has committed murder or a schedule 15 offence, and schedule 15 of the Criminal Justice Act (2003) lists over 150 offences (see relevant documents section)
Committed means convicted of, found not guilty by reason of insanity of, or found unfit to plead and to have done the act.
Was sentenced under section 37 or to more than 12 months imprisonment, and includes both guardianship orders and hospital orders, whether restricted or not.
Note a sentence of 52 weeks does not qualify as this is less than 12 months. If a sentence of more than 12 months is suspended, the individual is multi-agency public protection arrangement eligible while they are still subject to probation supervision.
Whose eligibility has not ended, eligibility ends with expiry of the sentence of imprisonment, so an individual who has been released on license may be eligible when an unrestricted patient becomes informal, so if a section 37 is discharged onto SCT, he remains multi-agency public protection arrangement eligible until the period of SCT ends when a restricted patient is absolutely discharged, so conditionally discharged patients are eligible.
10.1.3 Category 3: other dangerous offenders
Cautioned for or convicted of an offence, it need not be a schedule 15 offence.
Which indicates that he is capable of causing serious harm, serious harm is defined as:
“An event which is life threatening and, or traumatic, from which recovery, whether physical or psychological, can be expected to be difficult or impossible.”
The risk of which requires multiagency management. Active multi-agency management would enhance the risk management plans of the lead agency.
10.1.4 Category 4: terrorist offenders
A person falls within this category if:
- they are required to comply with the notification requirements set out in part 4 of the Counter Terrorism Act (2008)
- they have been convicted of a relevant terrorist offence and received a qualifying sentence or disposal for that offence
- they have been found to be under a disability and to have done the act charged or found not guilty by reason of insanity (or equivalents in Scotland and Northern Ireland) of a relevant terrorist offence with a maximum sentence of more than 12 months and received a hospital order (with or without restrictions) or guardianship order under Mental Health Act (1983) for that offence or
- they have committed an offence and may be at risk of involvement in terrorism-related activity (discretionary category 4): a person will be subject to notification requirements under part 4 of the Counter Terrorism Act (2008) if they are aged 16 or over and have been convicted (or found to be under a disability and to have done the act charged or found not guilty by reason of insanity) of an offence under section 41 or section 42 of the Counter Terrorism Act (2008) and who receive a qualifying sentence, a hospital order or a guardianship order
A relevant terrorist offence is an offence listed in schedule 19ZA of Criminal Justice Act (2003), a corresponding service offence, or an offence with a terrorist connection. An offence with a terrorist connection is one that the court has determined has been aggravated by having a terrorist connection under section 31 of the Counter Terrorism Act (2008) or the court has determined to have a terrorist connection under:
- section 69 of the Sentencing Code
- section 238(6) of the Armed Forces Act (2006)
- section 30 of the Counter Terrorism Act (2008)
- section 32 of the Counter Terrorism Act (2008)
A qualifying sentence includes:
- imprisonment for a term of 12 months or more (including indeterminate sentences), a sentence of 52 weeks is less than 12 months and would not therefore qualify an offender for category 4
- detention in youth detention accommodation for a term of 12 months or more (including indeterminate sentences); the whole term of a detaining and training order (DTO) is used to determine whether it is a qualifying sentence
- a suspended sentence with a term of 12 months or more, an offender has committed an offence and may be at risk of involvement in terrorism-related activity (discretionary category 4) if:
- the person has either:
- a conviction for any offence (current or historic, within the UK or abroad)
- received a formal caution (adult or young person) or reprimand and warning (young person) for any offence
- been found not guilty of any offence by reason of insanity; or- been found to be under a disability (unfit to stand trial) and to have done any act charged against them
- and the responsible authority believes that they may be or become involved in terrorism-related activity. This risk does not have to relate to the offence for which they received the disposal in paragraph above. The offence can be any offence. It does not have to be related to terrorism and may have been committed abroad. Discretionary category 4 offenders will be identified by Counter-Terrorism Police and the Probation Service National Security Division
- the person has either:
10.2 Appendix B levels of multi-agency public protection arrangements management and risk
Levels of management under multi-agency public protection arrangements (MAPPA). The multi-agency public protection arrangement guidance states that the central question in determining the correct multi-agency public protection arrangement level is:
“What is the lowest level of case management that provides a defensible risk management plan?”
The appropriate level of management correlates with level of risk but is not determined just by risk.
The level of risk is the likelihood of serious harm happening:
- low: evidence does not suggest a likelihood
- medium: there are identifiable indicators; harm is unlikely unless there is a change in circumstances
- high: potential event could happen at any time, and the impact would be serious
- very high: imminent risk of serious harm, potential event is more likely than not to happen imminently, and the impact would be serious
Level 1 cases are those for whom the risks can be managed effectively by the lead agency. Information sharing and discussions between agencies may still be warranted, but it is not necessary to refer the case to a level 2 or 3 multi-agency public protection arrangements meeting.
Level 2 cases are those in which either:
- the offender is assessed as posing a high or very high risk of serious harm
- the risk level is lower, but the case requires the active involvement and coordination of interventions from other agencies to manage the presenting risks of serious harm
- the case has been previously managed at level 3 but no longer meets the criteria for level 3
- multi-agency management adds value to the lead agency’s management of the risk of serious harm posed
Level 3 cases are those that meet the criteria for level 2 management, and in which the management issues require senior representation from the responsible authority and duty-to-cooperate agencies. This may be when there is a perceived need to commit significant resources at short notice or where, although not assessed as high or very high risk of serious harm, there is a high likelihood of media scrutiny or public interest in the management of the case and there is a need to ensure that public confidence in the criminal justice system is maintained.
Level 3 management is for cases that meet at least one of the following criteria:
- meet the criteria for level 2 and require senior representation and oversight by the responsible authority and duty-to-cooperate agencies to commit significant resources at short notice
- meet the criteria for level 2 and require senior representation and oversight to maintain public confidence in the criminal justice system. This may be due to high levels of current national media scrutiny or public interest in the management of the case as a result of the nature of the offence or the identity of the offender or victim
- Have a national security dimension and require senior oversight by Counter Terrorism Police (CTP) or the Probation Service National Security Division (NSD). Cases will be identified in line with lead agency case allocation polices relating to Counter Terrorism Police and Probation Service National Security Division. Discretionary category 4 offenders, like Category 3 offenders, must be managed at level 2 or 3
- involve high risk offenders involved in serious organised crime
10.3 Appendix C multi-agency public protection arrangement end process
Offenders will cease to be multi-agency public protection arrangements (MAPPA) managed offenders in the following circumstances.
10.3.1 Category 1
When the period of notification expires. In the most serious cases, offenders will be subject to lifetime notification requirements.
10.3.2 Category 2
When the licence expires, the offender is absolutely discharged from the hospital or guardianship order or when the community treatment order expires. An offender on licence for a consecutive or concurrent sentence will remain subject to multi-agency public protection arrangements until the whole sentence has expired. An offender does not remain automatically subject to multi-agency public protection arrangements as a result of post sentence supervision.
10.3.3 Category 3
When a level 2 or 3 multi-agency public protection arrangements meeting decides that the risk of harm has reduced sufficiently, or the case no longer requires active multi-agency management.
10.3.4 Category 4
For offenders subject to notification requirements, when the period of registration expires; for offenders at risk of involvement in terrorism related activity, when they no longer require multi-agency management; for other category 4 offenders, when the licence expires, the offender is absolutely discharged from the hospital or guardianship order or when the community treatment order expires. An offender on licence for a consecutive or concurrent sentence will remain subject to multi-agency public protection arrangements until the whole sentence has expired. An offender does not remain automatically subject to multi-agency public protection arrangements as a result of post sentence supervision.
All category 1, 2 and 4 offenders managed at level 2 or 3 who are coming to the end of their notification requirements or period of licence must be reviewed and considered for registration as a category 3 or discretionary category 4 offender. Registration as a category 3 or discretionary category 4 offender should only occur if they meet the criteria and continue to require active multi agency management.
10.4 Appendix D recording on SystmOne
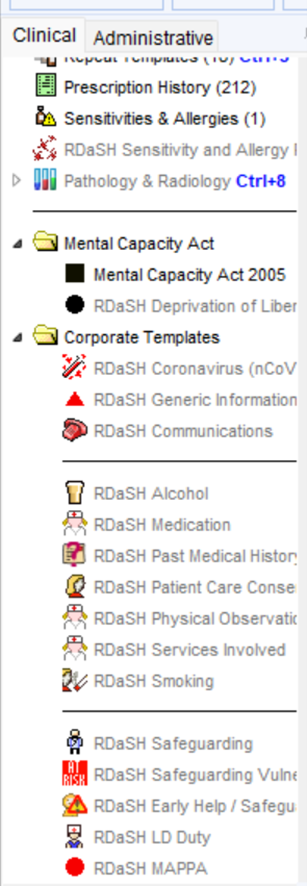 Access in the patient record, under clinical, on the left side.
Access in the patient record, under clinical, on the left side.
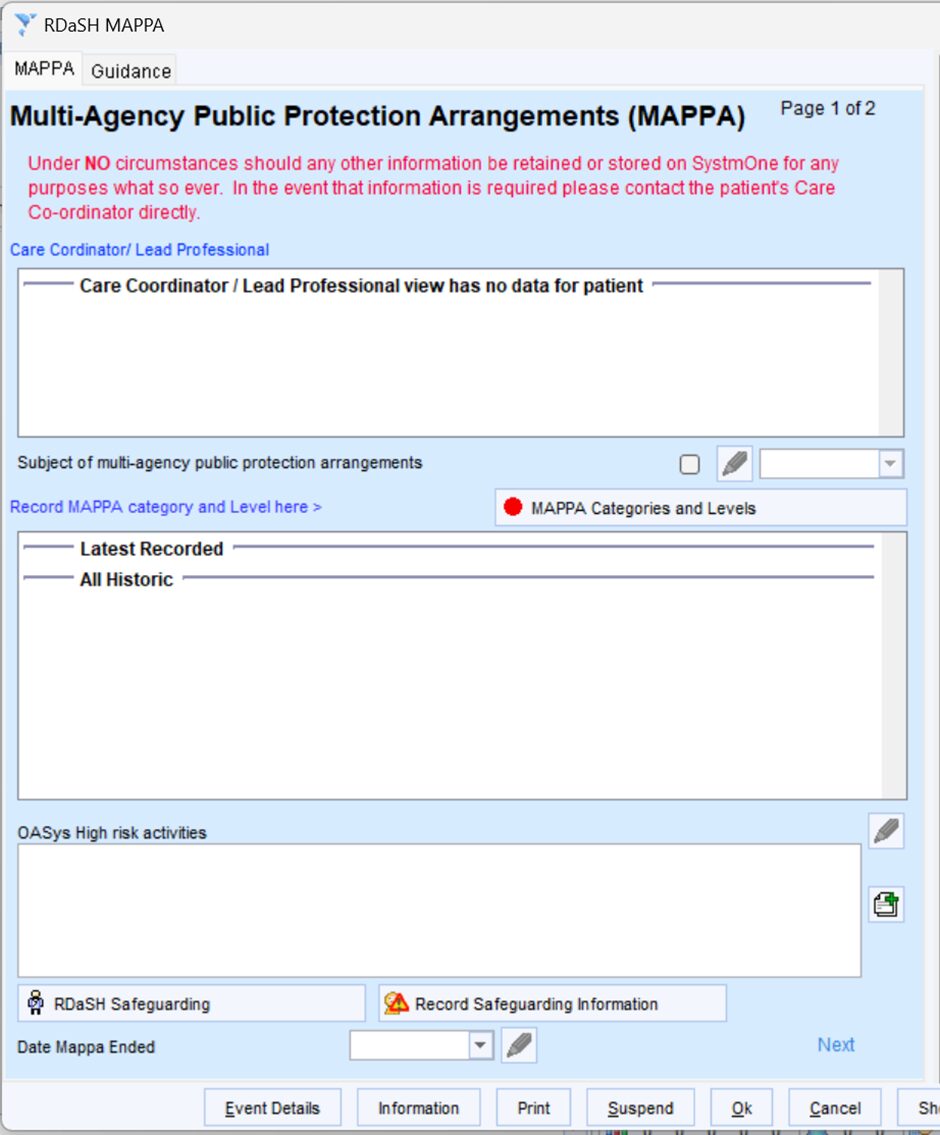
Tick the box and add the correct date of attendance at multi-agency public protection arrangements (MAPPA).
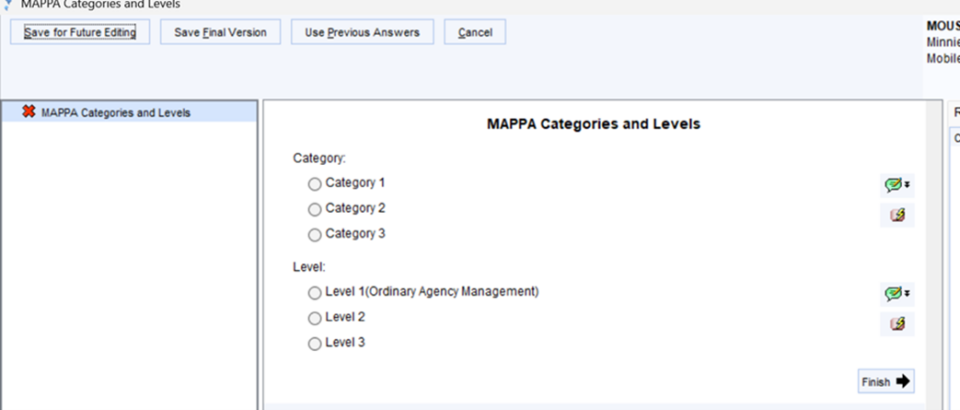
Fill in the relevant category and level of management as decided in the multi-agency public protection arrangements meeting.
Documentation is to be completed by the representative that attends the multi-agency public protection arrangements meeting. This is to be completed following each attendance.
10.5 Appendix E quick guide flow chart
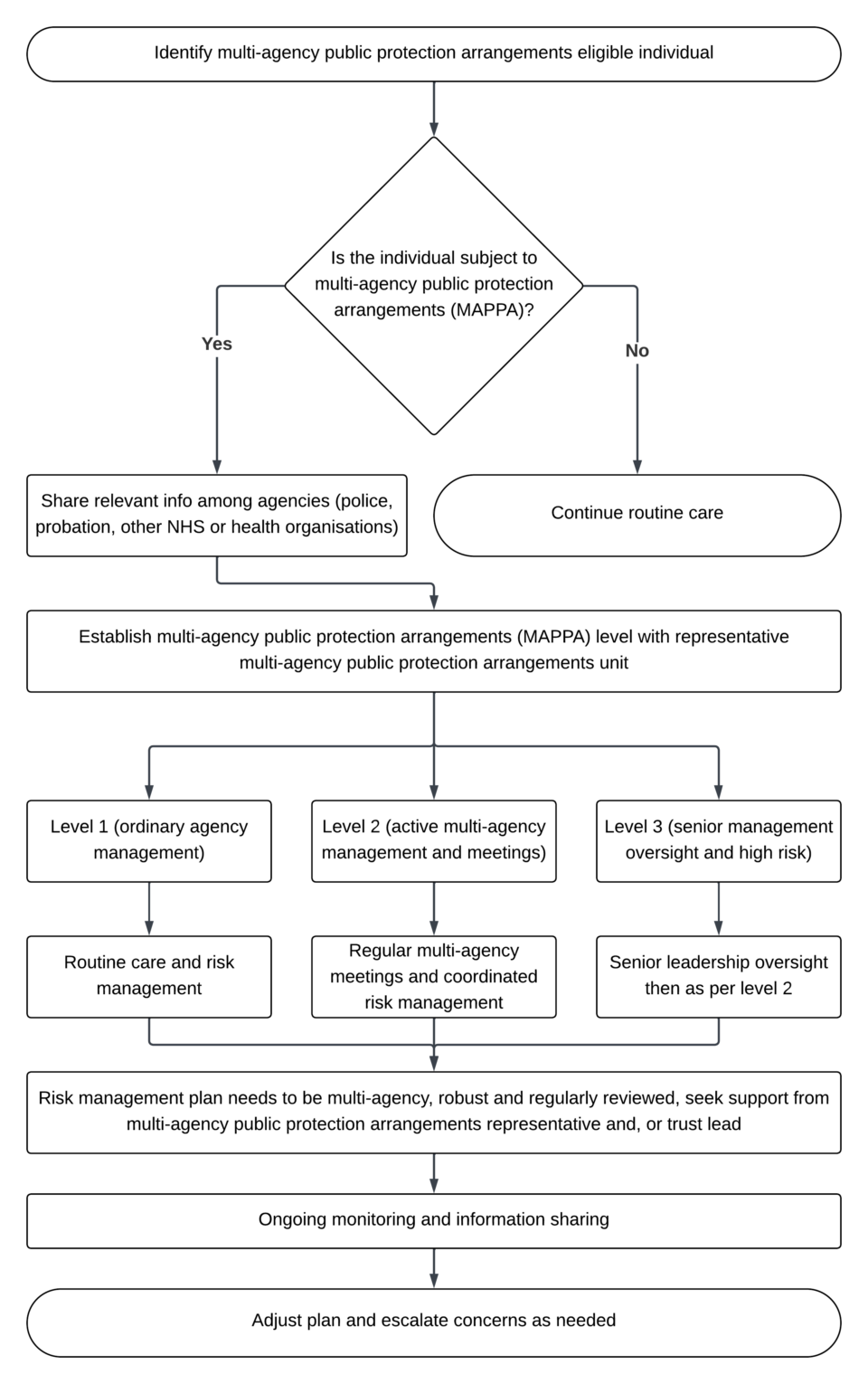
- Identify multi-agency public protection arrangements eligible individual.
- Is the individual subject to multi-agency public protection arrangements (MAPPA)?
- No: continue routine care.
- Yes: share relevant info among agencies (police, probation, other NHS or health organisations).
- Establish multi-agency public protection arrangements (MAPPA) level with representative Multi-Agency Public Protection Arrangements Unit.
- Level 1 (ordinary agency management): routine care and risk management.
- Level 2 (active multi-agency management and meetings): regular multi-agency meetings and coordinated risk management.
- Level 3 (senior management oversight and high risk): senior leadership oversight then as per level 2.
- Risk management plan needs to be multi-agency, robust and regularly reviewed, seek support from multi-agency public protection arrangements representative and, or trust lead.
- Ongoing monitoring and information sharing.
- Adjust plan and escalate concerns as needed.
10.6 Appendix F responsibilities, accountabilities and duties
10.6.1 The trust
The trust responsibilities, under multi-agency public protection arrangements guidance is to ensure that the risks posed by specified sexual and violent offenders are assessed and managed appropriately.
10.6.2 The chief executive
The chief executive has overall accountability and responsibility for multi-agency public protection arrangements within the trust. This function is delegated to the executive medical director and the chief nursing officer, who are responsible for ensuring operational managers are disseminating responsibility for the trust in respect of managing multi-agency public protection arrangements eligible individuals.
10.6.3 Care group quadrumvirate and trust wide multi-agency public protection arrangements representatives
To be aware of the multi-agency public protection arrangements policy, to ensure that sufficient colleagues have adequate knowledge of multi-agency public protection arrangements and to support colleagues in working within the policy.
10.6.4 Head of safeguarding and multi-agency public protection arrangements lead for the trust
To provide a single point of contact for the responsible authority for operational and case related matters. Providing case-specific advice or guidance to clinical colleagues on the interface with multi-agency public protection arrangements review and development of multi-agency public protection arrangements policy.
10.6.5 Head of information management and the Caldicott guardian
Supports the multi-agency public protection arrangements lead in relation to information sharing and confidentiality matters
10.7 Appendix G monitoring arrangements
10.7.1 Attendance at multi-agency public protection arrangements meetings and completion of multi-agency public protection arrangements eligibility forms
- How: attendance record, electronic patient records, completed eligibility forms.
- Who by: multi-agency public protection arrangements representatives, respective care groups,
- Reported to: annual multi-agency public protection arrangements strategic board and a copy is shared internally for dissemination as part of the trust safeguarding assurance.
- Frequency: annual.
Document control
- Version: 1.
- Unique reference number: 1114.
- Approved by: clinical effectiveness meeting.
- Date approved: 7 January 2026.
- Name of originator or author: deputy care group director children’s care group.
- Name of responsible individual: chief nurse.
- Date issued: 24 February 2026.
- Review date: 29 February 2029.
- Target audience: trust wide.
Page last reviewed: February 24, 2026
Next review due: February 24, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem