1 Policy summary
The prevent policy describes organisational responsibilities, around the prevent agenda in line with the prevent statutory duty issued for specified authorities in England and Wales on the duty in the Counterterrorism and Security Act (2015) to have due regard to the need to prevent susceptible people being drawn into terrorism.
The policy provides guidance to colleagues to help them identify susceptible individuals who may be at risk of being radicalised into violent extremism and to make sure that the appropriate safeguarding actions are taken where concerns for the individual are identified.
2 Introduction
2.1 What is prevent?
Prevent is part of the Home Office’s counter-terrorism strategy CONTEST, the aim of prevent is to stop people becoming terrorists or supporting terrorism. The trust is committed to ensuring susceptible individuals are safeguarded against being radicalised into violent extremism and supporting terrorism or becoming terrorists themselves.
CONTEST also includes the following elements in addition to prevent:
- pursue, to stop terrorist attacks, this means detecting and investigating threats at the earliest possible stage, disrupting terrorist activity before it can endanger the public and wherever possible prosecuting those responsible
- protect, to strengthen our protection against a terrorist attack by strengthening UK border security, strengthening the vulnerability of the transport network, increasing the resilience of the United Kingdom’s infra-structure, improve protective security for crowded places
- prepare, to mitigate the impact of a terrorist attack where it cannot be stopped. Prepare is based on an approach to emergency preparedness.
In order to deliver the prevent agenda, three national objectives have been identified:
- objective 1, respond to the ideological challenge of terrorism and the threat we face from those who promote it and tackle the causes of radicalisation
- objective 2,provide practical help to prevent people from being drawn into terrorism and ensure that they are given appropriate advice and support. Safeguard and support those most at risk of radicalisation through early intervention, identifying them and offering support
- objective 3, work with a wide range of sectors (education, health, social care, criminal justice, faith, charities, online) where there are risks of radicalisation which we need to address. Enable those who have already engaged in terrorism to disengage and rehabilitate
2.2 Why health care staff?
Prevent aims to protect those who are susceptible to exploitation from those who seek to get people to support or commit acts of violence. Healthcare colleagues are well placed to recognise individuals, whether patients or colleagues, who may be susceptible to radicalisation by extremists or terrorists. It is fundamental to our “duty of care” and falls within our safeguarding responsibilities.
3 Purpose
The purpose of this policy is to provide a framework for implementation of the Government’s prevent strategy. It also aims to identify the required action to be taken by trust colleagues in the event of any concerns about the potential risk to colleagues and susceptible patients, carers, or families being drawn into extremist activities. The principal objectives are:
- ensure that all trust colleagues, are aware of how to safeguard and support susceptible individuals, whether colleagues or patients, who they feel may be at risk of being radicalised by extremists
- ensure appropriate systems are in place within the trust for colleagues to raise concerns if they think this form of exploitation is taking place
4 Scope
The prevent agenda is relevant to all our colleagues, including volunteers, particularly those who work with susceptible people.
For further information about responsibilities, accountabilities and duties of all employees, please see appendix A.
5 Procedure
5.1 Quick guide
5.1.1 Consent
- Concern that someone is potentially susceptible to radicalisation.
5.1.2 Generic information
- If there is any immediate risk of harm call the police on 999 or the counterterrorism hotline on 0800 789 321.
5.1.3 Minimum content
- If no immediate harm contact the nurse consultant for safeguarding as the trust prevent lead or Safeguarding team for advice using rdash.safeguardingadults@nhs.net.
5.1.4 Timely entries
- Prevent lead or Safeguarding team will triage all referrals and assess whether the concern needs to be referred to the police prevent team
5.1.5 Letters
- If appropriate, a referral will be advised to channel panel for consideration.
- If not appropriate, patient risk assessment and care plan to be updated.
- Document on SystmOne.
- Complete an IR1.
- If the concern relates to a colleague contact HR using rdash.askhr@nhs.net and the prevent lead or Safeguarding team using rdash.safeguardingadults@nhs.net.
5.2 The process of exploitation
It is suggested that there is no single profile or indication of a person who is likely to become involved in terrorist-related activity. To date there is no universally accepted view of why individuals become involved.
The factors surrounding exploitation are many and they are unique for each person. The increasing body of information indicates that factors thought to relate to personal experiences of susceptible individuals affect the way in which they relate to their external environment.
In this sense, susceptible individuals may be exploited in many ways by radicalisers who target the vagaries of their susceptibility. Contact with radicalisers is also variable and can take a direct form, for example, face to face, or can happen indirectly through the internet, social networking or other media. More commonly this will occur through a combination of the above.
5.3 Internet
Islamist and extreme right-wing radicalisers fully exploit the power and speed of the internet to promote their narratives, influencing extremists within our own communities to disrupt our way of life through acts of violence. They groom the susceptible and the young to join or support their cause, inspiring people within our own communities to harm others.
Susceptible individuals may be exploited in many ways by radicalisers, and this could be through leaflets, direct face to face contact, or increasingly through the internet, social networking or other media.
The power of the internet in the radicalisation process cannot therefore be underestimated and radicalisers are making ever more sophisticated use of social media to spread their extremist messages and ideologies.
The internet provides a platform for extremists to promote their cause and encourage debate through websites, internet forums and social networking. It is a swift and effective mechanism for disseminating propaganda material and mobilising support but is not always easy or possible to monitor or regulate.
Trust colleagues should be aware of anyone making frequent unwarranted visits to websites showing extremist images and speeches or providing access to material from those involved in the radicalisation process and how they should raise their concerns.
A dedicated website to report suspected terrorism or suspicions that some may be involved in terrorism is available at reporting suspected terrorism.
5.4 Contact with radicalisers
It is generally more common for susceptible individuals to become involved in terrorist-related activity through the influence of others. Initial contact may be via peers, siblings, other family members or acquaintances, with the process of radicalisation often being a social one. Such social interaction takes place in a range of unsupervised environments such as gyms or cafés, in private homes and via the internet.
Access to extremist material is often through leaflets and local contacts. However, the internet plays an important role in the communication of extremist views. It provides a platform for extremists to promote their cause and encourage debate through websites, internet forums and social networking, and is a swift and effective mechanism for disseminating propaganda material.
Healthcare organisations should be aware of anyone making frequent visits to websites showing images such as armed conflict around the world and providing speeches and access to material from those involved in the radicalising process.
5.5 Use of extremist rationale (often referred to as “narrative”)
Radicalisers usually attract people to their cause through a persuasive rationale contained within a storyline or narrative that has the potential to influence views. Inspiring new recruits, embedding the beliefs of those with established extreme views and, or persuading others of the legitimacy of their cause is the primary objective of those who seek to radicalise susceptible individuals.
5.6 What factors might make someone vulnerable?
In terms of personal vulnerability, the following factors may make individuals susceptible to exploitation. None of these are conclusive in themselves and therefore should not be considered in isolation but in conjunction with the circumstances and any other signs of radicalisation.
5.6.1 Identity crisis
Adolescents or adults at risk who are exploring issues of identity can feel both distant from their parents or family and cultural and religious heritage, and uncomfortable with their place in society around them. Radicalisers can exploit this by providing a sense of purpose or feelings of belonging. Where this occurs, it can often manifest itself in a change in a person’s behaviour, their circle of friends, and the way in which they interact with others and spend their time.
5.6.2 Personal crisis
This may, for example, include significant tensions within the family that produce a sense of isolation of the susceptible individual from the traditional certainties of family life.
5.6.3 Personal circumstances
The experience of migration, local tensions or events affecting families in countries of origin may contribute to alienation from UK values and a decision to cause harm to symbols of the community or state.
5.6.4 Unemployment or under-employment
Individuals may perceive their aspirations for career and lifestyle to be undermined by limited achievements or employment prospects. This can translate to a generalised rejection of civic life and adoption of violence as a symbolic act.
5.6.5 Criminality
In some cases, a susceptible individual may have been involved in a group that engages in criminal activity or, on occasion, a group that has links to organised crime and be further drawn to engagement in terrorist-related activity.
5.6.6 Grievances
The following are examples of grievances which may play an important part in the early indoctrination of susceptible individuals into the acceptance of a radical view and extremist ideology:
- a misconception and or rejection of UK foreign policy
- a distrust of western media reporting
- perceptions that UK government policy is discriminatory (for example, counterterrorist legislation)
5.6.7 Other factors
Similarly, to the above, the following have also been found to contribute to susceptible people joining certain groups supporting terrorist-related activity:
- ideology and politics
- provocation and anger (grievance)
- need for protection
- seeking excitement and action
- fascination with violence, weapons and uniforms
- youth rebellion
- seeking family and father substitutes
- seeking friends and community
- seeking status and identity
5.7 Referral process
Where there are concerns that there is imminent danger to either the individual or to public safety then the police should be contacted directly by phone on 999 in addition to the standard process being followed.
If concerns about potential radicalisation are identified about a person that uses trust services, then the flow diagram included at appendix C outlines the process to be followed. Colleagues also have a duty of care to report potential radicalisation of family members of the person using trust services or any member of the public to the police who will then follow up with their prevent process.
If there are concerns about the potential radicalisation of colleagues, the trust’s human resources (HR) department must be contacted for advice using rdash.askhr@nhs.net and support following a discussion between the relevant senior manager and nurse consultant for safeguarding. Any internal processes or forms of investigation will be deferred if a police investigation is in progress to ensure there is no risk of compromising criminal proceedings.
In either case, if the first step in the process would place the individual at greater risk or could result in them taking terrorist action against the public as they feel that they have been discovered, these concerns should be escalated directly to the prevent lead within the organisation, or to the Safeguarding team. All information shared will be treated in the strictest confidence and will be shared on a need-to-know basis.
Prevent concerns or referrals should be discussed with the prevent lead or safeguarding team and a referral will be made dependent on a risk assessment based on the information available. The prevent lead may seek further guidance form the police prevent lead before advising a referral into the channel process.
The prevent concern should be entered on the trust’s incident reporting system as a prevent alert and categorised appropriately.
Where the trust receives an enquiry from the police, from the police prevent lead or other constabulary officers, this will be directed to the trust prevent lead or Safeguarding team and the trust will aim to progress this enquiry within 3 days of receipt.
Where a concern is identified relating to a child, the child protection process will be followed. Safeguarding children policy
All concerns, discussions and advice should be documented in line with trust policy.
6 Channel panel
Channel panel is a multi-agency process, much like safeguarding adults or children, where partner agencies share expertise and resources to create a bespoke support package for susceptible individuals.
If a patient is accepted into the channel process, involved colleagues can be expected to be asked to become involved in the process, share relevant information and attend the multi-agency channel panel if appropriate. Colleagues will be supported by a member of the safeguarding team who are standing panel members.
Colleagues must cooperate fully with channel panel, continue to support the patient to manage identified risks and to engage with the channel process. Channel is a consensual process whereby agreement from the patient is fundamental to the provision of interventions. The patient is therefore a key partner in the process and colleagues must seek to empower the individual to play an active role in support planning processes.
7 Training implications
The trust supports a consistent and proportionate approach to raising awareness of prevent as part of the wider safeguarding agenda which involves working with the NHS England’s prevent training and competencies framework to provide clarity on the level of training required for healthcare workers by identifying colleagues that require basic prevent awareness and those who need to be compliant with workshops to raise awareness of prevent (WRAP).
These sessions will ensure that staff are:
- aware of their professional responsibilities, particularly in relation to the safeguarding of adults at risk and children
- familiar with the trust’s relevant protocols, policies and procedures
- aware of whom they should contact to discuss concerns
- aware of the processes and support available when they raise a concern
Individual training matrices within electronic staff record will reflect the level of training the colleague is required to undertake.
7.1 Training needs analysis
7.1.1 Workshops to raise awareness of prevent (WRAP) train the trainer
- Employee groups requiring training: PREVENT WRAP trainers.
- How often should this be undertaken: Once.
- Length of training: 2 days.
- Delivery method: Face to face.
- Training delivered by whom: External trainers.
- Where are the records of attendance held: Electronic staff record system (ESR).
7.1.2 Workshops to raise awareness of prevent (WRAP)
- Employee groups requiring training: All clinical colleagues and colleagues who work with patients on a regular basis.
- How often should this be undertaken: 3 yearly.
- Length of training: 1 to 1 and half hours.
- Delivery method: E-learning.
- Training delivered by whom: Electronic learning for health
- Where are the records of attendance held: Electronic staff record system (ESR).
7.1.3 Prevent basic awareness
- Employee groups requiring training: All non-clinical colleagues.
- How often should this be undertaken: 3 yearly.
- Length of training: 1 to 1 and half hours.
- Delivery method: E-learning.
- Training delivered by whom: Electronic learning for health
- Where are the records of attendance held: Electronic staff record system (ESR).
8 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
8.1 Privacy, dignity and respect
The NHS constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
As a consequence the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
8.1.1 How this will be met
There are no additional requirements in relation to privacy, dignity and respect.
8.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
8.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005) (section 1).
9 Links to any associated documents
10 References
- Department for Health (2010) Building Partnerships Staying Safe
- Department of Health (2014) The Care Act
- Department of Health and Social Care (2022) NHS Prevent Training and Competencies Framework
- HM Government (2015) Counterterrorism and Security Act
- HM Government (2018) Contest: The United Kingdom’s Strategy for countering Terrorism
- HM Government (2022) Channel and Prevent Multi-Agency Panel (PMAP) Guidance
- HM Government (2023) Prevent and Channel Duty Guidance
11 Appendices
11.1 Appendix A Responsibilities, accountabilities and duties
11.1.1 Chief executive
Chief executive has ultimate accountability for ensuring robust systems are in place to ensure compliance with legal and regulatory obligations in relation to prevent.
11.1.2 Executive director of nursing and allied health professionals
The executive director of nursing and allied health professionals takes delegated accountability from the chief executive for ensuring the trust has effective systems and processes in place to meet the trusts responsibilities under prevent.
11.1.3 Nurse consultant for safeguarding
Nurse consultant for safeguarding is the trusts prevent lead. They are responsible for ensuring that appropriate training provision is made available to colleagues within the trust, with support from Learning and development. The prevent lead (or safeguarding team in the prevent leads absence) is the first point of contact for colleagues who believe that they have identified a concern about a patient which identifies them being at risk of radicalisation. The prevent lead is responsible for ensuring that quarterly prevent returns are submitted to NHS Digital.
11.1.4 Managers
Managers are responsible for ensuring that colleagues are undertaking training that is appropriate to their role, making arrangements for colleagues to be released from their duties in order to undertake training.
11.1.5 Trust colleagues
All trust colleagues (including volunteers) are responsible for undertaking training at a level appropriate to their role and for responding to and reporting any concerns that suggest that an individual may be at risk of radicalisation, in line with this policy.
11.2 Appendix B Monitoring arrangements
11.2.1 Prevent training compliance
- How: Training data.
- Who: Nurse consultant for safeguarding.
- Reported to: Safeguarding assurance group and NHS Digital.
- Frequency: Quarterly.
11.2.2 Prevent concerns raised
- How: Number of concerns reported via the IR1 system.
- Who: Nurse consultant for safeguarding.
- Reported to: Safeguarding assurance group and NHS Digital
- Frequency: Quarterly.
11.3 Appendix C Raising a prevent concern
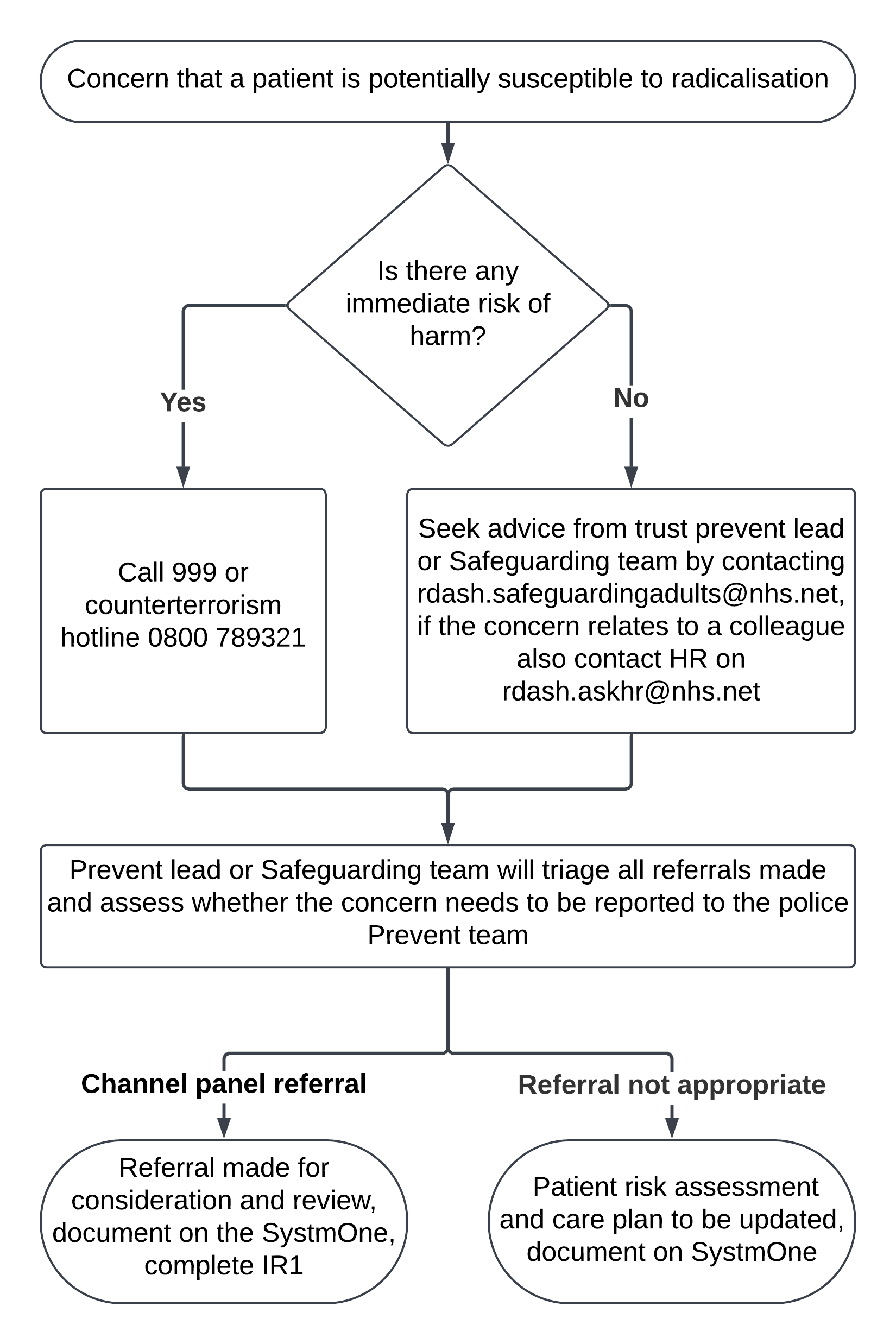
- Concern that a patient is potentially susceptible to radicalisation.
- Is there any immediate risk of harm?
- yes, call 999 or counterterrorism hotline 0800 789 321
- no, Seek advice from trust prevent lead or Safeguarding team by contacting rdash.safeguardingadults@nhs.net, if the concern relates to a colleague also contact HR on rdash.askhr@nhs.net
- Prevent lead or Safeguarding team will triage all referrals made and assess whether the concern needs to be reported to the police Prevent team.
- Channel panel referral. Referral made for consideration and review. Document on the SystmOne. Complete IR1.
- Referral not appropriate. Patient risk assessment and care plan to be updated. Document on SystmOne.
Document control
- Version: 6.
- Unique reference number: 155.
- Approved by: Clinical policy review and approval group.
- Date approved: 7 May 2024.
- Name of originator or author: Nurse consultant.
- Name of responsible committee or individual: Chief nurse.
- Date issued: 21 May 2024.
- Review date: 31 May 2027.
- Target audience: All trust colleagues.
Page last reviewed: September 08, 2025
Next review due: September 08, 2026
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem