1 Policy summary
The aim of the primary care mental health service (PCMHS) is to implement care through promoting wellbeing, prevention, and enablement of the patient group. Adopting a no wrong door approach, reflecting wherever patients seek their support they will be seamlessly guided to the most appropriate service rather than referred to another part of the mental health system. The purpose is to balance the patient seeking contact as and when needed, aiming to prevent illness or a worsening of symptoms. This reflects access to care not just when the patient is ill but according to the need to maintain wellbeing. This approach will encourage the patient to maintain individual responsibility for their health, wherever possible and appropriate.
2 Introduction
Traditionally, mental health services have a complex series of pathways and teams. The use of differing referral criteria, standards and processes create a system that is complex for those working within the system and for patients.
The NHS long term plan (NHS England and NHS Improvement, 2019) made a renewed commitment to improve and widen access to care for adults needing mental health support.
The Community Mental Health Framework for Adults and Older Adults (2019) focusses on putting community at the centre of community mental health services. Local areas were supported to redesign and reorganise core community mental health teams to move towards a new place-based, multi-disciplinary service across health and social care aligned with primary care networks (PCNs).
Since November 2022, a clearly defined model (appendix C) was created to show how people with a serious mental illness could be supported in their recovery.
Individuals and communities can maximise their health and wellbeing potential utilising new and existing community assets via an integrated care system approach. The patient’s journey will be to access the right care, support and treatment at the right time and to have a clear journey, not be passed around the health system. Patient journeys are to be considered as “step-up”, “step-down” or “step out” or “move-across” to the most appropriate intervention rather than the notion of referral and discharge, thus removing the barriers patients currently experience between primary and secondary care.
Where a patient is in a service that is not right for them, we will navigate them to the appropriate service or support.
Primary care networks are based on GP registered lists, typically serving natural communities of around 30,000 to 50,000. They are small enough to provide the personal care valued by both patients and GPs, but large enough to have impact and economies of scale through better collaboration between practices and others in the local health and social care system. Included within these primary care networks are more specific clinical functions, the provision of mental health care being one of them. (NHS England)
The introduction of the primary care mental health service (PCMHS) will incorporate the following:
- the introduction of primary care network mental health practitioners (MHP), along with mental health and wellbeing triage coaches (MHWBTC) where applicable, in the Rotherham, Doncaster and North Lincolnshire primary care networks through the new additional roles reimbursement scheme (ARRS).
- establishing the primary care mental health hub (PCMHH) aligned as per primary care network commissioning, which is tabled in appendix D
The primary care mental health service operates a model of delivery akin to general practices meaning all people registered to a general practitioner (GP) will be able to access the service (where they meet the eligibility criteria) without traditional GP referrals. As many mental health conditions are dynamic in terms of severity, longevity, and complexity, it is expected that people will have their needs met via self-management or community support without needing specialist mental health clinical input. Times will exist where the person needs to re-access clinical support services, and this should be easy and frictionless; joint working will see a number of people re-access support at a point where their condition has not deteriorated as significantly as in previous episodes of care (NHS Sheffield, September 2021).
The primary care mental health service works as an integrated part of a primary care network. In collaboration with GP’s, social care, voluntary, community and social enterprise (VCSE) providers, patients, family members and carers and wider specialist mental health teams work to support good physical, psychological and social wellbeing for the primary care network population, while ensuring responsive access to patients with the most complex of presentations.
3 Purpose
This purpose of this policy is to ensure that all colleagues working within the primary care mental health service, including additional roles reimbursement scheme (ARRS) roles, have a full understanding of the processes and procedures to follow to ensure a quality service that provides safe and effective care for our patients.
The purpose of the primary care mental health service is to improve coordination and collaboration of services. The aim of the team is to:
- provide an inclusive community based-offer, integrating community mental health services with primary care networks.
- remove traditional barriers between primary care mental health, specialist mental health and voluntary, community and social enterprise mental health provision, through new models of care, moving away from referral and discharge systems that lead to cliff edges.
- help prevent individuals from falling between gaps in services, such as those whose needs are higher than what talking therapies can offer but do not meet the traditional thresholds for specialist mental health teams; or those who have not engaged with specialist mental health services as they require support to reach these interventions. To overcome this, evidence-based interventions will be provided at a primary care network level for people with serious mental illness and complex emotional needs (traditionally defined as personality disorder).
- work in partnership with commissioned voluntary, community and social enterprise services, in order to:
- provide better care to people already receiving mental health support in the community, and
- increase access to community-based support services
- support people with severe mental illness (SMI) to access and receive a comprehensive physical health check across Rotherham, Doncaster and North Lincolnshire, making every contact count (MECC) principle
4 Scope
This document will apply to all Rotherham, Doncaster, and South Humber NHS Foundation Trust colleagues including substantive, temporary, and locum, of all grades and disciplines, working on behalf of the primary care mental health service and should be read in conjunction with the more detailed primary care mental health standard operating procedure.
For further information about responsibilities, accountabilities and duties of all employees, please see appendix A.
5 Procedure
5.1 Quick guide
5.1.1 Patient entry protocol into general practice (primary care)
- Patients contact general practice for support with their mental health or co-morbid presentation.
- Care navigators or reception within surgeries direct patients to the mental health practitioners (MHP) or mental health wellbeing triage coach (MHTC) where in place.
To note, patients in crisis should not be booked in with the mental health wellbeing triage coach or mental health practitioners, referrals should be made to crisis service via the agreed crisis referral route.
5.1.2 First contact
- The care navigator will book patients seeking support with their mental health with the mental health wellbeing triage coach (where applicable) or the mental health practitioner where triage is not in place (If deemed appropriate care navigators can directly send the patient the DIALOG scale via text (SMS) to be completed pre appointment).
- PHQ or GAD and DIALOG is completed in full at first contact point.
- If the patient has a follow-up appointment (seen more than once) “read code xal0u” to be entered for first contact and DIALOG+ undertaken in full to develop a care plan.
- Signpost to appropriate support or refer or book for further brief interventions with mental health practitioner.
- Patients care to be transferred as required (signposting, “step across” or “step up”) for example to NHS Talking Therapies.
- Patient to be stepped out of primary care mental health service (PCMHS) if no further support is required by the mental health practitioner (end of intervention). Any patient being stepped up to the Primary Care Mental Health team must have a completed DIALOG+ in place if they have undertaken an initial appointment with the mental health practitioner.
5.1.3 Primary care mental health practitioner (MHP) intervention
- Max 4 sessions of brief interventions can be provided by the mental health practitioner “read code xazrh” to be entered for patients follow-up contact.
- A full DIALOG scale should be undertaken. ReQoL-10 and goals-based outcomes (GBOs) can be completed as well if felt to be clinically appropriate before transition of care.
- Patient to be stepped out of primary care mental health service if no further support is required by the mental health practitioner (end of intervention).
- If further support is required then patient can be stepped up to the appropriate mental health service, for example mental health or NHS Talking Therapies via the no wrong door method ensuring the transfer of care is seamless.
- Referral to specialist mental health services can also be made where deemed appropriate via agreed referral route, the no wrong door methodology is instigated, and a seamless transition put in place, no need for further referral and waiting
5.1.4 Step up to primary care mental health hub
- Routine referrals should be electronically referred to the primary care mental health hub. The hub admin to register patient on SystmOne (if not already registered) and seamlessly book an appointment (no further action or follow-up should be required by the patient) and they are regularly updated on progress of appointment status.
- At point of referral the national 4-week wait pathway will begin.
- DIALOG scale to be completed by mental health practitioner if patient is stepped up. Primary Care Mental Health team to complete a DIALOG scale if one is not received electronically or linked to the record. Complete safety plan if required.
- If deemed appropriate discuss referrals and decisions made at multidisciplinary team meeting (MDT).
- Step patient into appropriate intervention or pathway if suitable for Primary Care Mental Health team and allocate to relevant caseload within first 7 days of referral.
- Complete goals-based outcomes (GBO) measure if clinically appropriate (within 4 weeks of referral).
- Complete ReQoL-10 if clinically appropriate (within 4 weeks of referral).
- Review the DIALOG+ care plan if one already in place or undertake a review of the DIALOG scale and complete the DIALOG+ with the service user to create a care plan.
- DIALOG, ReQoL-10 and goals-based outcome interventions would be discussed at a multidisciplinary team if deemed appropriate as part of a review of care. Representatives from specialist mental health teams may need to be present.
- Review safety plan as required.
- Transfer the care of the patient from primary care mental health service if no further intervention required or step up to specialist mental health services or step across to NHS Talking Therapies.
5.1.5 Specialist mental health
- If deemed appropriate discuss at multidisciplinary team when someone is identified as requiring more intensive intervention and or support from specialist mental health services.
- Specialist mental health team representatives to be part of the primary care mental health service multidisciplinary team and decision-making.
- Referral required to step up patients care to the specialist mental health team, completed DIALOG scale and any other patient reported outcome measures (PROMs) to be shared.
- Interventions and support undertaken.
- Complete DIALOG scale along with any other patient reported outcome measures as deemed clinically appropriate (for example goals-based outcomes and ReQoL-10) before, during and after interventions, these are your paired outcome measures.
- Following interventions, navigate care as appropriate for example step down to primary care mental health service or NHS Talking Therapies (if requiring low-moderate level support) or step out to primary care if no further intervention is required.
6 Safe operating standards
Safe operating standards include:
- operating days and times
- minimum staffing levels
- on call and or duty manager provision of advice and support
Please either refer to your local working instruction or ask your team manager for details on the safe operating standards within your locality.
7 Roles and multidisciplinary team
The primary care mental health multidisciplinary (MDT) contains a range of colleague disciplines who act as an integrated team to meet the serious mental illness (SMI) and or complex needs of the population of the primary care network. Every member of the multidisciplinary team is pivotal in providing the care, support, and treatment interventions within the integrated team.
Multidisciplinary team roles are listed in appendix A and are not exhaustive. It is important to note that the roles in place and taking part in a multidisciplinary team may differ between localities.
8 Assessment
Documentation and processes should be proportionate and enable the delivery of high quality care. Assessments will vary according to the needs of the individual and the complexity of their needs. For people with less complex needs an assessment can be a relatively brief initial contact in which an understanding of the person’s current problems and a shared view of an intervention have been developed and agreed with them.
The intervention itself may comprise a simple, short advice session that enables the person to obtain help for themselves, initiation of a treatment with medication and subsequent follow-up, or perhaps no further help will be required. For people with more complex needs, the assessment will be more comprehensive, and may require multidisciplinary input and interventions are also likely to be multi-professional in nature.
A single trusted assessment approach will be undertaken, resulting in a cumulative assessment that is built on throughout the patient journey, avoiding the need for patients to repeat their stories. This is an approach where assessors carry out holistic assessment of need, avoids duplication and speeds up response time so that people can be stepped up or down in a safe and timely way. For details on tools that will support this approach please see section 13: clinical documentation.
Assessments will be layered, the first layer, completed by the primary care mental health service, will contain sufficient detail to assess need and risk; this layer will be kept as brief as possible whilst maintaining quality and safety. If a patients need is beyond what the primary care mental health service can support and they require step up to specialist mental health services, then another layer of assessment will be completed to evidence the need. On accepting the patient, specialist mental health teams would undertake the next layer and more complex end of the assessment as recognised as necessary, meaning only those patients whose needs require full mental health assessments to plan their care, receive one.
If someone is at acute risk of ending their life, a referral for crisis assessment should be made by email. Copies of email correspondence with single point of access (SPA) should be recorded in SystmOne or EMIS (as applicable). The email should be followed up with a call to ensure the referral has been received and actioned and document phone calls with single point of access services in the SystmOne and, or EMIS notes.
9 Care planning
Care planning and care coordination is reframed under the community mental health transformation in order to work for everyone, it will focus on improved outcomes and deliver place based integrated mental health care to people, this will be done through moving towards a personalised care approach. The community mental health transformation framework envisages a shift away from risk assessments and ineffective predictive approaches to safety planning and positive risk taking, with colleagues supported by managers and to do so under progressive, partnership clinical governance arrangements.
Assessment of risk and safety planning will form part of a wider care planning process. A personalised approach to managing risk is a key part of the personalised care and support planning process. Once risks are identified, through personalised conversations options are explored that are relevant to the individual to help mitigate the risk. Patients with certain markers of risk (for example frequent consultations, multiple psychotropic drugs and specific drug combinations) are further assessed and considered for referral to specialist mental health services (NCISH, September 2022).
Every person who requires support, care and treatment in the community should have a co-produced and personalised care plan that takes into account all of their needs, as well as their rights under the Care Act, and Section 117 of the Mental Health Act when required. The level of planning and coordination of care will vary, depending on the complexity of their needs. For people with more complex needs, who may require interventions from multiple professionals, one person will have responsibility for coordinating care and treatment. This key worker role can be provided by workers from different professional backgrounds. The care plan will include timescales for review, which should be discussed and agreed with the person and those involved in their care at the outset.
The use of DIALOG+ will support the personalised care approach and will become the care plan.
9.1 Safety or risk
Evidence shows that the safest care is care that is personalised and highly responsive. Clear themes include:
- high-quality care planning
- an understanding of risk and safety as dynamic within a comprehensive assessment
- meaningful engagement with families and carers
- communication and information sharing
- robust record-keeping; and effective multi-agency working
The National Confidential Inquiry into Suicide and Safety in Mental Health describes how, to make approaches to safety personalised and effective, assessments of (changing) personal and individualised risks should not be based on the use of tools and checklists. It is therefore important that assessment of risk forms part of a wider assessment, and that safety planning is built into the wider care planning process rather than being divorced from it. A personalised approach to managing risk is a key part of the personalised care and support planning process. Once risks are identified, through personalised conversations options are explored that are relevant to the individual to help mitigate the risk.
Locally, risks will be recorded and mitigated in two ways:
- risks to employees such as environmental risks, risks from pets and individuals will be documented as “alerts” in the electronic patient record (EPR) and will be visible from the patient home screen
- risk associated to the patient will be documented and mitigated as part of the DIALOG+ safety plan and personalised care planning
10 Interventions
Within the primary care mental health service specific interventions can be provided based on identified patient needs, some of which are listed below. The interventions and input available may differ slightly between localities.
- psychoeducation
- formulation
- motivational interviewing
- guided self help
- mindfulness and relaxation
- medication optimisation
- emotional regulation
- time limited cognitive behaviour therapy (CBT)
- advice and support
- signposting
- serious mental illness (SMI) annual health checks (North Lincolnshire only)
- annual dementia medication review (North Lincolnshire only)
11 Caseload management
Mental health practitioner (MHP) will not hold a caseload, interventions will be on an appointment basis only. Where brief interventions support is required via the mental health practitioner a maximum of 4 sessions should be delivered, anyone requiring additional sessions should be stepped up to the primary care mental health hub (PCMHH).
Caseload management for the primary care mental health hub will be monitored and managed via the SystmOne clinical system. Caseloads should be discussed as part of clinical and management supervision.
Where caseloads are not being maximised as per the general practice contracted activity, it is the responsibility of general practice and the trust to monitor monthly contacts and activity, escalations must be audited and discussed at contractual meetings and any concerns about staff capacity shared with the service manager for ongoing action.
12 Non-medical prescribing
There are a number of patient and service benefits relating to non-medical prescribing. This section applies to those who undertake non-medical prescribing as part of their role.
There will be access to non-medical prescribing within the primary care mental health service where applicable. Full responsibilities as set out by the trust can be found in the non-medical prescribing policy. In addition, roles and responsibilities for people undertaking non-medical prescribing within their role are set out in their governing bodies, code of conduct, and guidance by the royal pharmaceutical society.
Involvement from the non-medical prescribing (NMP) (prescribing advice and guidance and or intervention) will be discussed and agreed within GP surgeries.
- Additional roles reimbursement scheme (ARRS) staff working as non-medical prescribers must comply with the trust policy maintaining their declarations, competence and supervision.
- Non-medical prescribers are able to initiate, stop and monitor patient medication within their agreed formulary and appropriate to primary care.
Other holistic interventions could be considered to meet psychological, social and general holistic needs of the patient.
13 Clinical documentation
13.1 Clinical governance
The primary care mental health service (PCMHS) will deliver high quality care, effectiveness and ensure safety for the patients referred into their care. The primary care mental health service will follow risk and incident reporting, the principle of freedom to speak for colleagues and where necessary learning from incidents, whether near misses or actual.
The care, support and interventions that are provided by the primary care mental health service are delivered within a primary care community setting, where patients are low to moderate risk. Therefore documentation and processes will be proportionate and enable the delivery of high quality care. Please refer to the care planning section within this policy, as well as information on moving towards personalised care approach for further detail.
The primary care mental health service within each locality has clear clinical leadership, but there will also be a shared model of leadership amongst the different primary care networks. Please refer to your local working instruction for details of the leadership structures.
Clinical governance will be monitored through supervision arrangements, team meetings and multidisciplinary team meetings. Further monitoring is detailed within the monitoring arrangements in appendix B.
13.2 Data protection
Patient information will be used in accordance with the data protection regulations policy.
14 Safeguarding
The primary care mental health service works to the trust safeguarding adults policy and the trust safeguarding children policy and should escalate and report concerns accordingly.
Responding to safeguarding concerns:
- make an immediate evaluation of the risk and take steps to ensure that the adult or child is in no immediate danger
- where appropriate, call 999 for emergency services if there is a medical emergency, other danger to life or risk of imminent injury, or if a crime is in progress
- consider if there are other adults with care and support needs or children who are at risk of harm and take appropriate steps to safeguard them
- contact the trust safeguarding team for advice if required
- report the incident internally on the incident reporting system
- ensure all decision-making is recorded in the electronic patient records, using the safeguarding adult or safeguarding children templates
- all safeguarding concerns must be reported to the adult safeguarding team in the local authority or children’s social care on the same day that the concerns were identified. contact details can be found in the corresponding safeguarding policies
- safeguarding concerns should always be shared with a clinical lead and the practice. patients with safeguarding concerns should be discussed at the next available multidisciplinary team meeting
Colleagues are to adhere to the trust lone working policy and where applicable complete lone worker risk assessments with their line manager.
15 Training implications
Training and development will reflect local and national drivers including National Institute for Health and Care Excellence (NICE) guidance, the needs of the trust or local authority and individuals who use services.
Colleagues development needs will be identified and reviewed and appraised annually in line with the trust personal development review (PDR) policy.
The trust recognises that continuing professional development is a key element of ensuring the delivery of evidence-based quality services. Role development and scope of practice is also increasingly relevant to the provision of colleagues training and supervision.
All colleagues should refer to the trusts mandatory and statutory training policy.
Training in new approaches may be required as agreed by the trust.
16 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
16.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
As a consequence the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
16.1.1 How this will be met
All employees, contractors and partner organisations working on behalf of the trust must follow the requirements of this policy and other related policies, particularly those relating to information governance. All health employees must also meet their own professional codes of conduct in relation to confidentiality.
16.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure for that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
16.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act 2005 (section 1).
17 Links to any other associated documents
The Primary Care Mental Health team (including additional roles reimbursement scheme roles) policy should be read in conjunction with related policies which include:
17.1 NHS England guidance
- NHS long term plan
- The community mental health framework for adults and older adults NHS England primary care networks
17.2 Trust policies
- Corporate and local service induction policy
- Mandatory and statutory training policy
- Non-medical prescribing policy
- Healthcare record keeping policy
- Safeguarding adults policy
- Safeguarding children’s policy
- Engagement and disengagement (mental health) policy
- Data protection regulations policy
- Lone working policy
18 References
- NHS England, Community Mental Health and NHS Talking Therapies for anxiety and depression, Annexes: National guidance to support seamless and person centred access to appropriate mental health care, page 16, July 2023
- NHS long term plan
- NHS Sheffield primary and community mental health service, service operational policies (SOPs), version 1.8, September 2021
- The community mental health framework for adults and older adults, prepared by: NHS England and NHS Improvement and the National Collaborating Central for Mental Health
- The National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH), Safer Services: A toolkit for specialist mental health services and primary care, University of Manchester, Healthcare Quality Improvement Partnership (HQIP)
19 Appendices
19.1 Appendix A responsibilities, accountabilities and duties
19.1.1 The trust
The trust has a duty of care and a duty of confidentiality to ensure that all aspects of healthcare record keeping are properly managed. The trust must adhere to the legislative, statutory, and good practice guidance requirements relating to healthcare records management.
19.1.2 The chief executive
The chief executive has overall accountability and responsibility for healthcare records within the trust. This function is delegated to the executive medical director and the executive director of nursing and allied health professionals, who are responsible for driving high quality standards of healthcare record keeping.
19.1.3 The trusts executive medical director
The trust’s executive medical director (and trust Caldicott Guardian) plays a key role in ensuring that NHS and partner organisations comply with current national guidance and relevant legislation regarding the handling and safeguarding of patient identifiable information. The Caldicott guardian will advise employees on matters relating to the management of patient identifiable information, for example where issues such as the public interest conflicts with duties such as maintaining confidentiality.
19.1.4 Senior managers of the trust
Senior managers of the trust are responsible for the quality of the healthcare records that are generated by all trust employees to ensure patient safety and quality service delivery.
19.1.5 Head of information management and business intelligence
Head of information management and business intelligence will advise the trust on how to maintain an efficient and effective patient information system, which complies with all the data collections required within the NHS.
19.1.6 All trust colleagues
All trust colleagues who come into contact with patients, are seen by doctors, nurses, allied health professionals, pharmacists, psychologists, bank colleagues and agency workers, students and volunteers. All are expected to ensure that each person coming into their care and their carers are treated with dignity and respect.
Members of the multidisciplinary team including external agencies, the patient and their family or carers should be aware of and involved in their care and treatment within the primary care mental health service in a timely manner.
All clinical and non-clinical colleagues involved in the care and treatment of a patient within the primary care mental health service, should ensure local and national guidance in relation to this is adhered to.
19.1.7 Multidisciplinary team roles
The roles listed below are not exhaustive and it is important to note that what roles are in place and taking part in a multidisciplinary team may differ between localities and may also change as the primary care mental health service is a developing service.
19.1.8 Service manager, clinical lead, cognitive behaviour therapy lead
Service manager or clinical lead or cognitive behaviour therapy lead; will aim to offer within each individual primary care network:
- overall clinical leadership in terms of the multidisciplinary team approach and strive for clinical efficiency, effectiveness and safety for people with severe or complex mental health needs, in the primary care setting
- will be the focus for contacts with external agencies
- will offer clinical supervision and line management for some roles within the primary care mental health hub
The clinical lead will also offer some clinical intervention according to:
- their professional background and expertise
- coordinate between the primary care networks
- ensuring there is service consistency
- sharing clinical expertise across the whole network
19.1.9 Mental health practitioners
Mental health practitioners mental health practitioners (MHP) are clinically registered practitioners; mental health nurses, mental health social workers or allied health professionals. The team will work alongside primary care network colleagues (with the population needs of the primary care network determining exact skill mix) to meet the needs of those with serious mental illness in line with the new mental health framework. The role of the mental health practitioner is a more specialist role than triage or gatekeeping. Depending on population needs and expertise they may directly undertake non-medical prescribing, social work interventions or evidence based psychosocial interventions in conjunction with other team members (NHS Sheffield, September 2021).
These roles should support people with complex mental health needs, rather than people for whom NHS talking therapies provision would be suitable. Mental health practitioners or mental health and wellbeing triage coaches should not be treating cases of anxiety or depression, which are more appropriately seen in NHS Talking Therapies (NHSE, 2023).
Mental health practitioners will be employed by the trust but be fully embedded into the primary care networks via a service agreement. This arrangement will maximise the opportunity to integrate two different organisations and working cultures, in an area where seamless transfers of patient care are particularly critical.
A primary care network must comply with the following requirements:
- the roles must: be embedded within the primary care networks core network practices and be fully integrated within the multidisciplinary team delivering healthcare services to patients
- have access to other healthcare professionals, electronic “live” and paper-based record systems of the primary care networks core network practices, as well as access to admin or office support and training and development as appropriate
- have access to appropriate clinical supervision and administrative support
19.1.10 Mental health and wellbeing triage coaches
Some primary care networks may have mental health and wellbeing triage coaches (MHWBTC) attached to them. The role of the mental health and wellbeing triage coaches is to work closely between the primary care mental health service, social prescribing and the mental health practitioners (MHP) to identify low or moderate support needs and signpost or coordinate the most appropriate route of care including Talking Therapies formerly improving access to psychological therapies (IAPT)) and the voluntary, community and social enterprises. People who present as needing more than talking therapies will be moved into an appointment with the mental health practitioner and an appropriate route of treatment and support will be identified including medicines management and escalations into the primary care mental health hub.
The mental health and wellbeing triage coaches would support anyone of working age presenting with a mental health need, they would not be expected to support anyone; in crisis, aged under 18, already under secondary or acute mental health services, with an eating disorder, with attention deficit hyperactivity disorder (ADHD),
or open to child adolescent mental health service (CAMHS).
19.1.11 Mental health nurse
A mental health nurse working within the primary care mental health service is instrumental in promoting and delivering evidence-based care for service users with mental health conditions within primary care. They will independently carry out assessments as trusted assessors and care plan interventions. Where appropriate, following assessment and formulation, liaise and signpost to teams within the community including social care and the voluntary sector, community mental health teams and addictions services.
19.1.12 Mental health social worker
Mental health social worker The social worker will provide social work service in the primary care community setting, offer interventions including:
- person led assessments
- risk assessment (within the context of primary care)
- support social care planning
- promote service user recovery
- promote social inclusion
19.1.13 Non-medical prescribers
Non-medical prescribers (NMP) Any prescribing completed by a healthcare professional other than a doctor or dentist. Clinician with non-medical prescribing skills will be registered with the trust to prescribe and will be included on the trust non-medical prescriber database, have their own non-medical prescriber folder and will adhere to the trust non-medical prescriber policy.
Full details on responsibilities and accountabilities can be found within the non-medical prescriber policy.
19.1.14 Clinical psychologist and psychotherapist
The clinical psychology team work with people on a wide range of psychological difficulties in mental and physical health. They bring enhanced skills of being able to provide formulation, review and interventions to support complex needs such as characteristics of personality disorder, complex cases and trauma informed practice.
19.1.15 Clinical associate psychologist
The clinical associate psychologist (CAP) work under the supervision of clinical psychologists and can provide support for complex stable individuals or those with intermediate level needs; presentations they support include anxiety, depression, personality disorder, post traumatic stress disorder (PTSD) and complex post traumatic stress disorder. Clinical associate psychologists are trained in assessment, formulation and intervention, which they deliver one to one with patients. Clinical associate psychologist will also support the development of group work activities as part of a range of interventions as well as support teams in a psychological way using their skills to offer a safe and supportive reflective space and helping the team think more psychologically.
19.1.16 Mental health wellbeing practitioner
The main responsibilities of Mental health wellbeing practitioner (MHWP) are to deliver evidenced based psychologically informed interventions to people with moderate to severe mental health problems and help support adults to receive the right care. The mental health wellbeing practitioner roles offer wellbeing-focused psychologically informed interventions for serious mental health problems for adults individually and in groups, as well as support their families and carers.
19.1.17 Occupational therapist
The occupational therapists support a patients’ recovery, helping those who have difficulties carrying out day-to-day activities due to disability, illness, trauma, ageing and a range of long term conditions. The occupational therapist will consider all of the patient’s needs, physical, psychological, social and environmental.
19.1.18 Peer support worker
Peer support workers are people who use their lived experience of mental health challenges to support others, they can help a person to maintain their ongoing community needs and engagement beyond formal clinical treatment to support their wellbeing and provide inspiration for their recovery. Peer support workers may be employed directly by trust or hosted within voluntary, community and social enterprise (VCSE) organisations given their strength and placement to local communities. These roles are of significant benefit to supporting the service to engage with, learn from and to adapt how services are provided. Peer support workers do not provide clinical care.
19.1.19 Community connector, social prescriber and link worker community connectors
Community connectors may be employed by the local authority, primary care or our voluntary, community and social enterprise (VCSE) partners and link between services. Community connectors can advise on the local offer of voluntary, community and social enterprise support available in each primary care network; they play a key role by giving people time, focusing on “what matters to me” and taking a holistic approach to people’s health and wellbeing in order to connect them to appropriate community groups and services. Depending on a persons need, a community connector may only need to provide advice and signposting, whilst others may require a short-term package of support to help their social needs, such as social activities, debt, housing, education, training, employment, or family support.
19.2 Appendix B monitoring arrangements
19.2.1 Compliance with the policy
- How: through discussion during supervision at team meetings.
- Who by: team managers.
- Reported to: exception reported to care group leadership meetings.
- Frequency: as required.
19.2.2 Patient experience: complaints
- How: review of complaints.
- Who by: Patient Safety and Investigations team
- Reported to: care groups.
- Frequency: monthly.
19.2.3 Patient experience: Care Opinion
- How: review of Care Opinion.
- Who by: service managers.
- Reported to: care groups.
- Frequency: monthly.
19.2.4 Patient outcome and experience measure
- How: completion of paired outcome or experience measure tools (for those requiring more than one contact), to be recorded on the electronic patient record by colleagues assessing and delivering interventions to patients, to help measure quality and effectiveness of the intervention or treatment offered to improve patients mental health and wellbeing.
- Who by: report would be compiled by the performance or Commissioning for Quality and Innovation (CQUIN) team for organisational monitoring. This data also flows into the Mental Health Services Data Set (MHSDS) for national monitoring.
- Reported to: care group performance meetings.
- Frequency: monthly.
19.2.5 Improved access to services
- How: adherence to the access and waiting times standards from initial contact with any primary, secondary care or other service to appropriate mental health care, for patients who need further support after initial contact.
- Who by: this would be recorded in the electronic patient record by colleagues seeing patients within the primary care mental health service. Report would be compiled by the Performance team for organisational monitoring. This data also flows into the Mental Health Services Data Set for national monitoring.
- Reported to: care group performance meetings.
- Frequency: monthly.
19.2.6 Improved access to services
- How: expanding patient access by 5% each year in all transformed and non-transformed community mental health teams. Referrals and contacts recorded by colleagues working in the primary care mental health service and specialist community mental health teams in the electronic patient record.
- Who by: report would be compiled by the Performance team for organisational monitoring. This data also flows into the Mental Health Services Data Set for national monitoring.
- Reported to: care group quality meetings by performance.
- Frequency: monthly.
19.3 Appendix C community mental health model
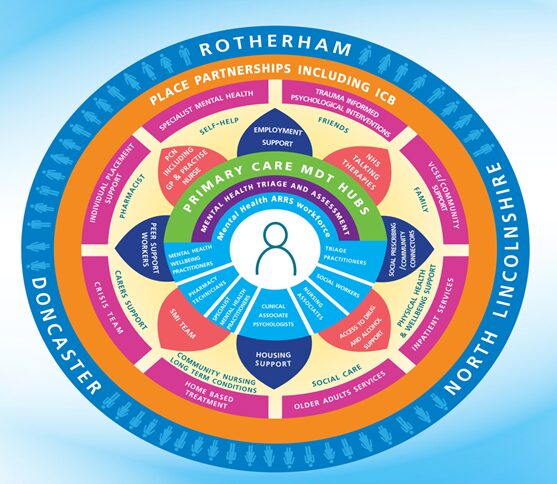
19.3.1 Rotherham, Doncaster, and North Lincolnshire
Place partnerships including integrated care board (ICB):
- specialist mental health (self-help)
- trauma informed psychological interventions (friends)
- voluntary, community and social enterprise (VCSE) or community support (family)
- inpatient services (physical health and wellbeing support)
- older adults services (social care)
- home based treatment (community nursing long term conditions)
- crisis team (crisis support)
- individual placement support (pharmacist)
These encompass:
- employment support
- NHS Talking Therapies
- social prescribing or community connectors
- access to drug and alcohol support
- housing support
- serious mental illness team
- peer support workers
- primary care networks including GP and practice nurses
19.3.1.1 Primary care multidisciplinary team hubs
19.3.1.1.1 Mental health triage and assessment
Mental health additional roles reimbursement scheme (ARRS) workforce consists:
- mental health wellbeing practitioners
- pharmacy technicians
- specialist mental health practitioners
- clinical associate psychologists
- nursing associates
- social workers
- triage practitioners
19.4 Appendix D primary care networks
19.4.1 Rotherham
- Maltby Wickersley
- Central North
- Health village and Dearne valley
- Rother Valley South
- Raven
- Wentworth
19.4.2 Doncaster
- North primary care network
- South primary care network
- East primary care network
- Doncaster primary care network
- Central primary care network
- Northwest Doncaster
19.4.3 North Lincolnshire
- West primary care network
- East primary care network
- North primary care network
- South primary care network
19.5 Appendix E abbreviations
| Term | Meaning |
|---|---|
| ARRS | Additional role reimbursement scheme |
| CAPs | Clinical associate psychology (trainee role) |
| CAMHS | Child adolescent mental health service |
| EMIS | Clinical IT system used by some GP practices |
| GP | General practitioner |
| LTP | NHS long term plan |
| MDT | Multidisciplinary team |
| MHP | Mental health practitioner |
| MHWBTC | Mental health and wellbeing triage coach |
| NHSE | NHS England improvement |
| PCMHS | Primary care mental health hub |
| PCMMH | Primary care mental health hub |
| PCN | Primary care network |
| SMI | Serious mental illness |
| SPA | Single point of access (Sheffield Health and Social Care NHS Foundation Trust) |
| SystmOne | Clinical IT system used by the service and some GP Practices in Sheffield |
| RDaSH | Rotherham, Doncaster and South Humber NHS Foundation Trust |
| VCSE | Voluntary, community and social enterprise |
Document control
- Version: 2.
- Unique reference number: 1072.
- ratified by: clinical effectiveness group.
- Date ratified:
- Name of originator or author: service manager, community mental health directorate (Rotherham, Doncaster and North Lincolnshire).
- Name of responsible individual: chief operating officer.
- Date issued: 30 October 2025.
- Review date: 30 September 2028.
- Target audience: all colleagues working within the primary and community mental health service.
Page last reviewed: December 30, 2025
Next review due: December 30, 2026
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem