1 Introduction
The decision and procedure to resuscitate, or not when there is a valid do not attempt cardio-pulmonary resuscitation (DNACPR) decision in place for both adults and children within the trust are all in one manual. The introduction of, and rationale for, each procedure will be within the relevant chapter.
2 Purpose
The purpose of this manual and the linked procedure documents is to provide clear, concise guidance on managing, for both adults and children:
- the risks associated with resuscitation
- the systems in place to support effective resuscitation provision
- the deteriorating patient
- do not attempt cardio-pulmonary resuscitation (DNACPR) decision
- recommended summary plan for emergency care and treatment (ReSPECT)
The manual outlines the duties and responsibilities of the trust to comply with the relevant local and national legislation and guidance and monitor compliance with this manual so that an effective service is provided.
3 Scope
This manual applies to all managers with responsibilities derived from it, and all staff (clinical and non-clinical), including bank, agency and temporary staff who may need to summon help if they come in to contact with a patient, visitor or member of staff who becomes acutely unwell.
4 Responsibilities, accountabilities and duties
4.1 Chief executive
The chief executive is responsible for making arrangements to support the safe and effective implementation, monitoring and review of this policy manual.
4.2 Medical director and chief operating officer
These directors are responsible for implementation and monitoring of the policy manual within their areas of responsibility.
4.3 Consultants and medical officers
Consultants and medical officers in charge of patients’ care retain overall responsibility for the decisions relating to procedures within this policy manual.
4.4 Resuscitation Committee
The Resuscitation Committee are responsible for reviewing the trust’s assurance processes within this policy manual and to oversee the annual audit work plan adhering to the UK Resuscitation Council Quality Standards (see appendix A).
4.5 Resuscitation service
- Liaise with managers or modern matrons to formulate suitable staff training programmes to support effective implementation of this policy manual.
- Deliver training using the current national guidelines.
- Maintain a central record of training delivered and produce reports on training compliance.
- Discuss with the managers or modern matrons the approach to be taken with staff who do not successfully complete the training assessments.
- Act as specialist advisors to the trust on resuscitation and related matters.
- Produce an annual audit of resuscitation events, resuscitation equipment, choking incidents and do not attempt cardio-pulmonary resuscitation (DNACPR) or recommended summary plan for emergency care and treatment (ReSPECT) orders.
- Produce a quarterly audit report on the continual availability of equipment, see appendix D, emergency equipment required in healthcare areas.
- Facilitate policy and practice development and organisational learning as a result of audit.
- Support Managers in facilitating an environment where incidents are reviewed in an open and positive manner, involving staff at all levels in improving practice and promoting organisational learning
- Be available as a source of specialist advice and support to managers and staff, including incident debriefing.
- Represent the trust on the regional DNACPR working party and the Doncaster locality End of Life group as the DNACPR lead for the trust.
- Lead the review and updating of this policy.
4.6 Managers or modern matrons
- Disseminate, implement and monitor implementation of this policy manual within areas of responsibility.
- Facilitate, support and monitor ward or team managers in their responsibilities with regard to policy implementation and monitoring.
- Identify and allocate resources in order to comply with this policy manual.
- Make available appropriate and suitably maintained resuscitation equipment, maintaining up-to-date medical devices inventories in all areas of responsibility.
- Promote incident reporting and audit requirements as specified within the policy through local induction processes in all areas of responsibility.
- Facilitate an environment where incidents are reviewed in an open and positive manner, involving staff at all levels in improving practice and promoting organisational learning.
- Proactively seek advice and support from the resuscitation service.
4.7 Ward or team managers
- Facilitate effective local induction processes for all new starters
- Manage the process of releasing staff for training and updating at least annually in the skills relevant for their area, in line with the mandatory risk management training policy.
- Maintain staff training records for the area, including temporary, bank and agency staff.
- Proactively identify risks due to lack of training or resources to the manager or modern matron.
- Manage and maintain the resuscitation equipment within the area of responsibility via:
- an up-to-date medical devices Inventory
- signed and dated daily and weekly equipment check records (as per requirements set out in appendix D continual availability of equipment, see appendix D, emergency equipment required in healthcare areas), in line with the manufacturer’s recommendations; a record of these checks will be kept for 3 years
- report any equipment issues immediately to the manager or modern matron
- adequate stocks of disposable or single use parts of the resuscitation equipment required in that area, such as pocket masks, oxygen masks, airway tubes, defibrillator pads etc. to maintain continued functioning of the equipment by immediate replacement
- Maintain the equipment ready and available for use for another event as soon as practicable after a resuscitation attempt where the equipment is used.
- Make timely arrangements for staff involved in a resuscitation event to be supported, debriefed, and offered counselling as required in conjunction with the resuscitation officer.
- Facilitate an environment where incidents are reviewed in an open and positive manner, involving staff at all levels in developing policy and practice and promoting organisational learning.
- Proactively seek advice and support from resuscitation service.
4.8 Clinical and non-clinical staff
- Adhere and implement this policy manual within the scope of their job role (the resuscitation council expects all staff to recognise cardiac arrest, to commence cardiopulmonary resuscitation and call for help).
- Report any issues which affect the effective implementation of this manual to their manager, for example, access to training or equipment.
- Report all incidents as per the incident reporting policy including the use of the appropriate cardiac arrest report form.
- Maintain a personal record of their own training.
- Contribute to the review of incidents in an open and positive manner in order to improve practice and promote organisational learning.
5 Procedures
5.1 Resuscitation and the deteriorating adult procedure
5.1.1 Aim
The availability of suitable cardio-pulmonary resuscitation (CPR) is expected of healthcare services, and a service user has the right to expect such support from a healthcare provider. Therefore, it is recognised that employees of Rotherham Doncaster and South Humber NHS Foundation Trust (hereafter known as the trust) may be involved in resuscitation procedures in the course of their work.
As a provider of specialist mental health, learning disability and community services it is essential that the trust provides resuscitation at an appropriate level. For effective life support, standardised equipment, training, and protocols must be provided. Across the trust this provision will be determined by the location of the healthcare facility, the colleagues available and the type of healthcare provided and will at all times be supported by the local ambulance service.
This procedure outlines the systems in place in the trust to provide high quality resuscitation to its patients at all times.
5.1.1.1 Definitions
| Term | Definition |
|---|---|
| Cardiopulmonary resuscitation (CPR) | Cardiorespiratory arrest is defined clinically by unconsciousness in association with no established breathing pattern and no signs of life. |
| Do not attempt cardiopulmonary resuscitation order | Cardiopulmonary resuscitation is a combination of external chest compressions, artificial respiration, and defibrillation. It is undertaken to restore breathing and circulation in a person where these life-giving functions have failed. |
| Choking | Choking is the occlusion of the airway by a foreign body, causing the inability to breathe, it is a medical emergency and can, if not treated cause cardiorespiratory arrest. |
| Anaphylaxis | Anaphylaxis is a severe, life threatening, generalised, or systemic hypersensitivity reaction. |
| Mental capacity | The ability of an individual to make decisions regarding specific elements of their life. This is also sometimes referred to as “competence”. |
| Community life support | Community life support is resuscitation training that includes the recognition of cardiorespiratory arrest, how to provide external chest compressions and artificial respiration, how to deal with choking situation in adults and children, the manual handling of a patient in emergency situations and the introduction to defibrillation. |
| Immediate life support | Immediate life support is training that includes the recognition of the deteriorating patient and cardiorespiratory arrest, how to provide external chest compressions, artificial respiration, and defibrillation, and how to deal with a choking situation in adults and children. The course also includes the use of the early warning score, neurological observations, oxygen therapy, suction, the dangers of restraint and rapid tranquillisation. |
5.1.2 Procedure
5.1.2.1 Cardiopulmonary arrest prevention and the deteriorating patient
The resuscitation service will work alongside the medical director (physical health and wellbeing) to promote the importance of physical wellness and healthy lifestyles.
The trust will wherever possible promote the prevention of cardiopulmonary arrest occurring by monitoring and observing:
- physically unwell and deteriorating patients
- those being restrained both during and after the restraint
- those that have been given rapid tranquillisation
- those with Head injuries or possibility of head injury (unwitnessed fall)
- those who have been suspected of using a ligature
Physical observations for these patients will be taken in conjunction with the use of a track and trigger system the National early warning score 2 (NEWS2), a plan for vital signs monitoring that identifies which variables need to be monitored including the frequency of measurements, as advised by the Resuscitation Council, National Institute for Health and Care Excellence (NICE) and National Confidential Enquiry into Patient Outcome and Death (NCEPOD).
To work alongside the NEWS2 and neuro observations the resuscitation service has developed flow charts for both head injuries and ligatures. See appendix B.
5.1.2.2 Emergency lifesaving drugs
The provision of standardised medication to treat the deteriorating patient is vital, therefore, all inpatient areas carry drugs that can be given in emergency situations by a registered nurse, these drugs will be kept in stock medication cupboards, easily accessible at all times, stored with the appropriate paraphernalia to administer, and the appropriate flow chart displayed on the outside of the cupboard.
These drugs are:
- aspirin
- glyceryl trinitrate (GTN) spray
- naloxone
- glucagon or glucogel
- adrenaline
- oxygen
- salbutamol
When an emergency lifesaving drug is administered the following details must be recorded in the patient records:
- date
- time
- drug name
- strength
- dose
- route
- batch number
- expiry date
- along with the details of the patient’s presentation at the time of administration
See appendix C for flow charts for administration.
5.1.2.3 Equipment
The provision of suitable, standardised equipment is paramount in resuscitation so that colleagues are familiar, proficient and confident with the use of that equipment.
For areas revaluating the provision of resuscitation equipment within their areas the trust emergency equipment risk assessment must be used in conjunction with discussions with the resuscitation officer.
Details are shown in appendix D, equipment required in healthcare areas.
5.1.2.4 Initiation of and criteria for resuscitation
All patients, visitors, and colleagues who collapse within the vicinity of trust premises are to be resuscitated in line with this procedure. All patients being attended by a clinician, whether in hospital, healthcare unit or their own home, are to be actively and vigorously resuscitated, and suitable assistance called, unless they have a do not attempt cardio-pulmonary resuscitation (DNACPR) order in place, rigour mortis is present, or there are signs of decomposition. The temperature and pallor of the person’s skin should not be used as an indicator of the initiation of cardiopulmonary resuscitation (CPR).
In circumstances where colleagues think the casualty should have a DNACPR order, but doesn’t, full resuscitation is to be attempted until the emergency services arrives and takes over, or a recognised doctor issues orders to stop resuscitation efforts.
On finding someone collapsed, colleagues should immediately assess the casualty, using the danger, response, airway, breathing and circulation (DRABC) approach, and summon further assistance by initially shouting for help and activating any alarm systems in place. As soon as a medical emergency has been identified, then an ambulance will be summoned by all areas within Tickhill Road Hospital and Tickhill Road Site.
Dialling: 2222 on the internal phone system, state cardiac arrest, the caller will be given instructions by switchboard staff to enable the call to be transferred to the ambulance service.
- Great Oaks dialling: 9-999
- The Woodlands dialling: 9-999
- Swallownest Court dialling: 9-999
- All other areas dialling: 999
- Softphone: 999 goes straight through to emergency services
5.1.2.5 Relatives who choose to witness resuscitation attempts
The Resuscitation Council UK (RCUK) suggested that family members who witness the resuscitation process may have a healthier bereavement, as they will find it easier to come to terms with the reality of their relative’s death and may feel reassured that everything possible has been done. It is acknowledged that the reality of cardiopulmonary resuscitation may be distressing, but in the latest edition of RCUK’s advanced life support manual, the RCUK argues that:
“Many relatives want the opportunity to be present during the attempted resuscitation of their loved one.” (RCUK, 2021).
Each cardiac arrest situation needs to be taken on a case-by-case basis and if there is opportunity and time to invite family members and loved ones to witness the resuscitation process then this should be accommodated. However, as we know there are some situations this may be difficult, and therefore the appropriate support should be offered such as effective communication from one professional from the care team to speak with the family, provision of a suitable room to speak to family, breaking bad news and supporting the grief response, arranging viewing of the body and religious requirements, legal and practical arrangements as stated from the RCUK paper wherever possible.
In the community setting, where staff often visit patients alone, the trust support staff prioritising the clinical emergency first and if there is an opportunity after the event then to support the family.
5.1.2.6 Do not attempt cardio-pulmonary resuscitation orders
In line with the HSC 2000/028, the trust has adopted the Yorkshire and Humber region system whereby a patient or medical officer can withdraw the provision of resuscitation. The trust do not attempt cardio-pulmonary resuscitation (DNACPR) procedure can be found in the do not attempt cardiopulmonary resuscitation within the resuscitation manual. It is the responsibility of all colleagues to know which process is to be followed for DNACPR in their care group for example, the recommended summary plan for emergency care and treatment (ReSPECT) orders process or version 13 DNACPR.
5.1.2.7 Incident reporting, including external reporting requirements
All resuscitation attempts should be reported on the trust incident reporting system and by the completion of the cardiac arrest report form (appendix E) which must be received by the resuscitation officer’s email within 24 hours of the incident.
All serious (life threatening) sudden medical emergencies, for example, choking and anaphylaxis, and any emergency medical equipment failures should be reported using the trust incident reporting system. Patient safety incidents are required to be reported to the National Patient Safety Agency (NPSA), deaths to the coroner’s office and certain deaths to the care quality commission. Please see the incident management policy for details.
5.2 Do not attempt cardiopulmonary resuscitation (DNACPR) adult
5.2.1 Aim
The primary goal of medical treatment is to benefit patients, by restoring or maintaining their health as far as possible, thereby maximising benefit and minimising harm. If treatment fails or ceases to give a net benefit to the patient, or if a patient has competently refused the treatment, this goal cannot be realised and the justification for providing the treatment is removed.
Prolonging a patient’s life usually provides a health benefit to that patient. Nevertheless, it is not an appropriate goal of medicine to prolong life at all costs with no regard to its quality or the burdens of treatment on the patient. There are occasions when due to the nature of someone’s physical state, and quality of life, a decision may be made that in the event of that person experiencing a cardio-respiratory arrest, cardiopulmonary resuscitation would not be desirable. This includes circumstances where a patient is already dying and has a terminal illness. In these circumstances patients should be allowed to die peacefully and with dignity.
Under the provisions of the Mental Capacity Act (2005), patients with capacity can decide that the stage has been reached beyond which, for them, continued treatment aimed at prolonging life, although possible, would be inappropriate. Patients may have also utilised the provisions of the act to identify a point in the future after which they do not want treatment, including life sustaining, and refuse further interventions through an advanced decision. Please refer to the trust’s policy for advance statements and advance decisions
Under the provisions of the Mental Capacity Act (2005) where patients have no advance decision and lack capacity, all decisions about whether to provide treatment must be taken in a way that reflects their best interests. Under the act, patients have the right to appoint an attorney to make healthcare decisions on their behalf.
An attorney can only make life-sustaining treatment decisions if this is made explicit within the lasting power of attorney order. In these circumstances the attorney must always act in the donor’s best interests (Mental Capacity Act (2005) Code of Practice (2007)). Please refer to the trust’s Mental Capacity Act (2005) policy.
Where the patient who lacks capacity has no relative or friend to support life-sustaining decisions, the Mental Capacity Act (2005) has made provisions for the instruction of an independent mental capacity advocate to be consulted to support the best interest decision-making process. Please refer to the trust’s Mental Capacity Act (2005) policy.
Any assessment of best interests must include the patient’s clinical presentation and any current and previously expressed wishes and preferences. Where there is no information about their wishes or preferences, decisions must be consistent with and not contrary to their interests or rights. The emphasis on the individual’s interests means that it is important that resuscitation is discussed sensitively with patients who have capacity, and people close to patients who lack capacity including any nominated attorney. This can help people to understand why treatment is given and why, in some circumstances, it may be unable to provide any benefit.
Each case involves an individual patient with their circumstance, and it is important that these circumstances are central to each decision rather than applying the same decision to whole categories of patients. Unless a patient who lacks capacity has an appointed Attorney with explicit powers to make decisions regarding life-sustaining treatment, any decision not to attempt resuscitation is ultimately the responsibility of the medical officer in charge of the patient’s care (see definition section). Good practice however dictates that consultation should, whenever possible, take place with the other members of the team involved in the care of the patient. Provisions are made under the Mental Capacity Act (2005) and its Code of Practice (2007) for referring decisions to the Court of Protection should professionals’ judge that an Attorney is not acting in a donor’s best interest. Please refer to the trust’s Mental Capacity Act (2005) policy.
This procedure is based on the guidelines produced in 2016 by the British Medical Association (BMA), Royal College of Nursing (RCN) and Resuscitation Council (UK) and should be read in conjunction with this document. It is written with due regard for the requirements of the Mental Capacity Act (2005).
This procedure should be read in conjunction with the relevant professional standards and guidelines including the Nursing and Midwifery Council (NMC) publication Professional standards of practice and behaviour for nurses and midwives 2015 and the General Medical Council (GMC) publication, treatment and care towards the end of life; good practice in decision-making (July 2010).
This procedure should be read in conjunction with the Recommended Summary Plan for Emergency Care and Treatment (ReSPECT) South Yorkshire Integrated Care Board regional policy and the trust wide standard operating procedure.
5.2.1.1 Definitions
| Term | Definition |
|---|---|
| Cardiopulmonary resuscitation (CPR) | Cardiopulmonary resuscitation is a combination of external chest compressions, artificial respiration, and defibrillation. It is undertaken to restore breathing and circulation in a person where these life-giving functions have failed. |
| Do not attempt cardiopulmonary resuscitation (DNACPR) order | Do not attempt cardiopulmonary resuscitation is an order stating that a decision has been made either by the patient or medical officer in charge of their care that cardiopulmonary resuscitation (CPR) would have no clinical benefit or be wished for in this situation. It is essential that healthcare professionals, patients and those close to the patients understand that a decision not to attempt cardiopulmonary resuscitation applies only to cardiopulmonary resuscitation and not any other treatment that may be appropriate for example, antibiotics, analgesia, feeding, hydration, suction, treatment for choking and so on. |
| Medical officer in charge of patient care | In inpatient care this will be the patients named consultant and in the community the patient’s GP, unless an agreed service provision is in place. |
| Healthcare professional | A registered nurse, doctor, or allied healthcare professional. |
| Mental capacity | The ability of an individual to make decisions regarding specific elements of their life. This is also sometimes referred to as “competence”. |
| Mental incapacity | A person lacks sufficient capacity in relation to a matter if, at the material time they are unable to make a decision for themselves in relation to the matter because of an impairment of, or a disturbance in, the functioning of the mind or brain. This lack of capacity may be permanent or temporary. |
| Advance decisions to refuse treatment (ADRT) | A decision made by any person aged 18 years or over, whilst having mental capacity, to refuse specified life sustaining treatment or intervention at a later time, should they lose capacity to make such decisions. |
| Independent mental capacity advocate (IMCA) | An independent advocate appointed to support vulnerable patients who lack mental capacity and have no one appropriate to act on their behalf. Independent mental capacity advocates can also become involved if staff conclude that relatives or other carers may not be acting in a patient’s best interests. |
| Lasting power of attorney (LPA) | A legal document whereby an individual (the donor) authorises another person (the donee) to act on their behalf, in the event that the donor should lose the capacity to make their own decisions. This authority can be in respect of decisions regarding personal welfare and consent to medical treatment. In order to be valid a lasting power of attorney should be executed on the prescribed form and registered with the public guardian. If it applies to end of life decisions this must be clearly stated |
| Relevant other | For the purpose of this policy, the term “relevant others” is used to describe patient’s spouses, partners, relatives, carers (who are not acting in a paid, professional capacity), representatives, advocates, people with lasting power of attorney, independent mental capacity advocates and court appointed deputies and any other person deemed to have an interest in the wellbeing of the patient. |
| Young person | Within the context of this policy manual and procedures, the term young person refers to any patient aged 16 or 17 years of age. |
| Child | Within the context of this policy manual and procedures, the term child refers to patients who are under the age of 16. |
| Best interests | When a patient has been assessed as lacking capacity, anything done for, or decisions made on their behalf, should be done in their best interest. Best interests are assessed by healthcare professionals weighing up the treatment options in the context of the individual patient, once appropriate enquiries have been made of the patient (as far as is possible) and others. Best interest decisions include wider issues than medical issues. Mental Capacity Act (2005) Code of Practice. General Medical Council (2010). |
| Futility | When treatment is considered unable to produce the desired benefit because it cannot achieve its physiological aim, for example, there is no real prospect of restarting the heart and breathing for a sustained period of time. |
5.2.2 Procedure
5.2.2.1 Do not attempt cardiopulmonary resuscitation in inpatient areas
On admission to an inpatient area it is only necessary to discuss the cardiopulmonary resuscitation status of a patient and consider making a do not attempt cardiopulmonary resuscitation decision in the following circumstances:
- where the patient’s condition indicates that cardiopulmonary resuscitation is unlikely to be successful
- where successful cardiopulmonary resuscitation is likely to be followed by a length and quality of life which would not be in the best interests of the patient to sustain
- where cardiopulmonary resuscitation is not in accord with the recorded sustained wishes of a patient who has capacity
- where cardiopulmonary resuscitation is not in accord with a valid applicable written advance decision which demonstrates a patient’s informed, voluntary and competently made refusal, which relates to the circumstances which have arisen, is legally binding upon medical staff
In cases where a patient is admitted to a ward with an existing do not attempt cardiopulmonary resuscitation (DNACPR) order, this order will remain but must be reviewed on the day of admission and an entry made in the patients notes on the DNACPR template (see appendix K).
All patients admitted to an inpatient area should have their resuscitation status documented within the admission documentation, if they have a recommended summary plan for emergency care and treatment (ReSPECT) plan:
- RDaSH ReSPECT and DNACPR template. The template must be completed for all patients that have a ReSPECT plan and their Resuscitation status identified.
- a discussion with the patient (and, or those close to them, where appropriate) is only required if the medical decision is for DNACPR
- clinicians completing or reviewing a ReSPECT document must follow the ReSPECT procedure
Clinicians involved in these discussions must understand the framework for making decisions about resuscitation. It is essential to recognise whose decision it is, and to distinguish between the legal requirements and the clinical responsibilities. Conversations should focus on ensuring that the patient, or those closest to them are fully aware of the decision, rather than simply completing a DNACPR form. The only exception is when there is an advance decision to refuse treatment (ADRT) that specifically declines cardiopulmonary resuscitation (CPR).
See decision-making framework flowchart.
5.3 Child 18 years and under recommended summary plan for emergency care and treatment procedure
5.3.1 Aim
Within Rotherham Doncaster and South Humber NHS Foundation Trust (the trust) physically ill children under 18 years of age will be under the care of a consultant from a neighbouring acute trust. However, these children may be cared for within the community by trust services.
The document used to document the resuscitation status of a child under the age of 18 years is the recommended summary plan for emergency care and treatment (ReSPECT) document. Please see the ReSPECT procedure for emergency care planning and do not attempt cardiopulmonary resuscitation (DNACPR) decisions that have used this process.
The clinical circumstances that surround cardiorespiratory arrest in children differ from those of adults; the legal and ethical aspects also differ.
It is vital that when these agreements have been made that the child is offered the same treatment by all clinicians involved in their care.
The aim of this procedure is to ensure that trust colleagues are aware of their responsibilities surrounding the children and young peoples advanced care planning (CYACP) which is the children’s ReSPECT form.
The procedure aims to ensure a consistent approach for sharing the planned decisions for children across the trust and to ensure that decisions that have been made about children in other specialist services can transfer between the different services and localities of the trust and that the trust does not compromise patient care.
The procedure outlines the duties and responsibilities of the trust to comply with relevant legislation and guidance.
5.3.2 Definitions
| Term | Definition |
|---|---|
| Cardiopulmonary resuscitation | Cardiopulmonary resuscitation (CPR resuscitation) is a combination of external chest compressions, artificial respiration, and defibrillation. It is undertaken to restore breathing and circulation in a person where these life-giving functions have failed. |
| Do not attempt cardiopulmonary resuscitation order | Do not attempt cardiopulmonary resuscitation order (DNACPR) is an order stating that a decision has been made either by the patient or their carer with the medical officer in charge of their care it provides a summary of personalised recommendations for their clinical care in a future emergency in which they ae not able to make decisions or to express wishes, this may include cardiac arrest but is not limited to those events. This may also include the decision not to resuscitate. |
| Medical officer in charge of patient care | In inpatient care this will be the patient’s consultant and, in the community, the patient’s GP. |
| Healthcare professional | A registered nurse, doctor, or allied healthcare professional. |
| Child | Within the context of this procedure, the term child refers to patients who are under the age of 18 years. |
5.3.3 Procedure
If a child within the care of the trust children’s services has an existing recommended summary plan for emergency care and treatment (ReSPECT) from within another organisation, the lead trust clinician should liaise with the child’s consultant from the other organisation, the child and their family to discuss this and to ensure that circumstances have not changed and that is still current
5.3.3.1 Communication of the order
The lead trust clinician must ensure that all clinicians involved in the child’s care are aware of the order.
The order must remain with the child. Discussions should be held with the child if possible, and their parents as to the importance of ensuring the document goes with them when they are attending services, school etc.
Any child that has a child and young persons advance care plan (CYPACP) in place should have an alert added to SystmOne by the practitioner completing the recommended summary plan for emergency care and treatment (ReSPECT) trust template to alert multidisciplinary teams that the child or young person has a ReSPECT in place.
Also, the clinician should add a reminder (high priority category) stating that ReSPECT in place and where the electronic version is saved in the patient record.
The key clinician should also notify South Yorkshire Ambulance Service (YAS) for an alert to be flagged on their systems.
If the decision within the ReSPECT is that in the case of cardiopulmonary arrest that resuscitation will not take place, this needs to be clearly documented and shared with relevant parties. In the event of this decision being made the lead trust clinician will inform the trust medical director and share the ReSPECT document with them.
5.3.3.2 Presumption to resuscitate
“All patients being attended by a clinician, whether in hospital, healthcare unit or their own home, are to be actively and vigorously resuscitated and suitable assistance called, unless they have a recommended summary plan for emergency care and treatment (ReSPECT) that details otherwise. Where no decision has been made about cardiopulmonary resuscitation (CPR) before any subsequent cardiopulmonary arrest, and the express wishes of the person are unknown it is expected that colleagues will attempt resuscitation.”
However, the Resuscitation Council state the below, which does allow for some senior clinical decision-making.
“Where no explicit decision about cardiopulmonary resuscitation has been considered and recorded in advance there should be an initial presumption in favour of cardiopulmonary resuscitation. However, in some circumstances where there is no recorded explicit decision (for example a person in the advanced stages of a terminal illness where death is imminent and unavoidable, and cardiopulmonary resuscitation would not be successful) a carefully considered decision not to start inappropriate cardiopulmonary resuscitation should be supported.” (Resuscitation Council 2021)
Is it important to note that healthcare or nursing assistants must commence cardiopulmonary resuscitation if a ReSPECT form is not in place that details that resuscitation is not to be undertaken.
In circumstances where cardiopulmonary resuscitation has been initiated without the knowledge of an existing documented decision to not resuscitate, and this form is presented the continuation of cardiopulmonary resuscitation would be inappropriate however the decision to stop must come from a senior healthcare professional (doctor or registered nurse). If there is any doubt, cardiopulmonary resuscitation should continue until reviewed by the attending paramedic or doctor.
5.3.3.3 Review of the recommended summary plan for emergency care and treatment form
The recommended summary plan for emergency care and treatment (ReSPECT) form will be reviewed when the health needs or circumstances changes, although it Is good practice to review at least annually, and should be reviewed in each person’s individual situation.
5.4 Recommended summary plan for emergency care and treatment (ReSPECT)
This is a South Yorkshire Integrated Care Board policy, please refer to South Yorkshire Integrated Care Board ReSPECT policy.
6 Training implications
In adherence with the expectations of the Resuscitation Council UK, all colleagues should have basic knowledge and skills in resuscitation. All colleagues should be equipped to recognise cardiac arrest, to commence cardiopulmonary resuscitation (CPR) and call for help. All colleagues should attend, as a minimum, community life support (CLS) every 12 months.
All employees working in areas where physical restraint, rapid tranquilisation or seclusion may be required, will be trained to a level equal to the immediate life support (ILS) course of the Resuscitation council UK. This will be repeated every 12 months.
All employees working within areas with immediate access to a defibrillator will be trained to the equal level of the immediate life support course of the Resuscitation Council UK. This will be repeated every 12 months.
6.1 Enhancing clinical staff support in resuscitation training
Objective: our organisation is committed to empowering clinical colleagues through resuscitation training, ensuring everyone has equitable access to learning, support, and workplace inclusion. Our aim is to support clinical colleagues not only in training, but also in identifying and managing any clinical limitations appropriately.
Equality, Diversity and inclusion commitment: in alignment with the Resuscitation Council UK’s Diversity and Inclusion policy:
“Resuscitation council UK recognises the value of having a diverse group of people with a diversity of thinking and perspectives involved in the organisation” and “is committed to working with partners that represent all of society… ensures that all its officers, trustees, staff, instructors and other volunteers and consultants have equal opportunity to achieve their full potential.”
Resus council UK equal opportunities policy: this policy underpins our approach, affirming that training and support must be inclusive, fair, and reflective of diverse needs and perspectives.
Identification and risk assessment:
- clinical limitations identified during training (for example, physical, cognitive, sensory, or other) will be escalated to the colleague member’s line manager
- the line manager is responsible for conducting a tailored risk assessment to determine appropriate adjustments or accommodations in the workplace
Learning and development support:
- our Learning and Development team is dedicated to providing reasonable adjustments during resuscitation training. These may include assistive aids, alternative formats, extra time, or modified practical setups
- where adjustments are implemented, the Learning and Development team will communicate feedback to the line manager to facilitate consistent support beyond training
Escalation to senior resuscitation officer: if additional support or guidance is required, the trust’s senior resuscitation officer must be promptly contacted to offer further assistance and oversight.
6.1.1 Summary of roles and responsibilities
- Clinical staff: participate in training; disclose any limitations identified.
- Line manager: review limitations; conduct a risk assessment; implement workplace adjustments.
- Learning and development: provide reasonable adjustments during training; feedback outcomes to line management.
- Senior resuscitation officer: offer further assistance and oversight if required.
See colleague clinical limitations and reasonable adjustment risk assessment form (staff access only).
Basic training on do not attempt cardiopulmonary resuscitation (DNACPR) and recommended summary plan for emergency care and treatment (ReSPECT) will be within the community life support and immediate life support sessions. For clinicians who have such discussions within their job roles (includes some specialist nurses identified in the Resuscitation Committee), additional training is required (see DNACPR and ReSPECT sections)
The Yorkshire and Humber e-learning is an excellent source of information and can be used as a training resource in team meetings. It can also be used as an individual training resource and can be found on the trust eLearning platform.
6.1 All non-clinical and community clinical colleagues community life support training (includes do not attempt cardio-pulmonary resuscitation or recommended summary plan for emergency care and treatment)
- How often should this be undertaken: 12 months.
- Length of training: 3 hours.
- Delivery method: face to face.
- Training delivered by whom: resuscitation service.
- Where are the records of attendance held: electronic staff record (ESR).
6.2 All in-patient clinical colleagues immediate life support (ILS) training
- How often should this be undertaken: 12 months.
- Length of training: 3 hours.
- Delivery method: face to face.
- Training delivered by whom: resuscitation service.
- Where are the records of attendance held: electronic staff record (ESR).
6.3 Clinicians that have escalation plan discussions in care groups that have recommended summary plan for emergency care and treatment: e-learning
- How often should this be undertaken: one-off.
- Length of training: 40 minutes.
- Delivery method: e-learning, ReSPECT.
- Training delivered by whom: Resuscitation Council UK.
- Where are the records of attendance held: electronic staff record (ESR).
6.4 Clinicians that have escalation plan discussions in care groups that have recommended summary plan for emergency care and treatment
- How often should this be undertaken: one off and more if required.
- Length of training: 1 hour.
- Delivery method: face to face clinical supervision for additional sessions.
- Training delivered by whom: nurse consultant in palliative care. consultants in older peoples mental health.
- Where are the records of attendance held: electronic staff record (ESR).
As a trust policy, all colleagues need to be aware of the key points that the policy covers. Colleagues can be made aware through a variety of means such as:
- all user emails for urgent messages
- one to one meetings or supervision
- continuous professional development sessions
- posters
- daily email (sent Monday to Friday)
- practice development days
- group supervision
- special meetings
- intranet
- team meetings
- local induction
7 Monitoring arrangements
7.1 Policy implementation
- Policy implementation including:
- requirement for a documented plan for vital signs monitoring that identifies which variables need to be measured, including the frequency of measurement
- use of an early warning system within the trust to recognise patients at risk of deterioration
- actions to be taken to minimise or prevent further deterioration in patients
- how the trust documents that resuscitation equipment is checked, stocked and fit for use
- incident reports of resuscitation events
- incident reports of choking situation events
- staff training, as identified in the training needs analysis
- How: resuscitation audit.
- Who by: resuscitation officer.
- Reported to: quarterly and annually.
- Frequency: Resuscitation Committee.
8 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
8.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
As a consequence the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
8.1.1 How this will be met
There are no additional requirements in relation to privacy, dignity and respect.
8.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
8.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005) (section 1).
9 Links to any other associated documents
- Consent to care and treatment policy
- Clinical risk assessment and management policy
- Clinical skills policy
- Incident management policy
- Infection prevention and control
- Mandatory and statutory training policy
- Mental Capacity Act (2005) policy
- Medical devices management policy
- Slips, trips and falls for staff and visitors, prevention and management policy
- Rapid tranquillisation policy and guidelines (pharmacological management of violence)
10 References
- Resuscitation Council (UK) (2021) resuscitation guidelines
- Guidance, do not attempt cardiopulmonary resuscitation (DNACPR) and cardiopulmonary resuscitation (CPR) decisions
- Recommended Summary Plan for Emergency Care and Treatment (ReSPECT), Resuscitation Council UK
- Mental Capacity Act (2005)
- Advance decisions to refuse treatment guide
- Advance care planning, end of life care, Royal College of Nursing
11 Appendices
11.1 Appendix A Resuscitation Committee terms of reference
11.1.1 Name of committee or group
Resuscitation Committee.
11.1.2 Purpose
The purpose of this Resuscitation Committee is to review the trust’s assurance processes for resuscitation and to oversee the annual audit work plan taking into account UK Resuscitation Council Quality Standards.
11.1.3 Membership
The membership of the group would include:
- medical director (chair)
- nurse consultant, St John’s Hospice (deputy chair)
- lead learning and development facilitator, mandatory and statutory training
- chief pharmacist or a nominated deputy
- head of patient safety
- clinical representation from each care group as determined by the relevant associate nurse director
- medical representative
- allied health professional representative
- patient governor representative
- non-executive director
11.1.4 Attendance
All members, or a nominated deputy, from each care group should attend each meeting. Each care group representative should have a clinical background. In addition, other directors, senior managers and advisors will be invited to attend as and when required. Attendance will be recorded in the minutes of each meeting.
11.1.5 Quoracy
The chair or deputy chair and a clinical representative from each care group should be present. The senior clinical representative will be determined by the associate nurse director from each care group.
11.1.6 Meeting arrangements (frequency, chair, venue, administrative support arrangements)
Meetings shall be held 3 monthly. Administrative support will be provided by the executive medical director’s personal assistant.
11.1.7 Key responsibilities or objectives or duties or powers
These key responsibilities (KR) will be represented in the agenda responsibilities of the Resuscitation Committee as defined by the Resuscitation Council (UK) include:
- key responsibility 1: ensuring implementation and adherence to national resuscitation guidelines and standards
- key responsibility 2: defining the role and composition of the resuscitation team
- key responsibility 3: ensuring that resuscitation equipment for clinical use is available and ready for use
- key responsibility 4: ensuring that appropriate resuscitation drugs (including those for peri-arrest situations) are available and ready for use
- key responsibility 5: planning adequate provision of training in resuscitation
- key responsibility 6: determining requirements for and choice of resuscitation training equipment
- key responsibility 7: preparing and implementing policies relating to resuscitation and treatment of anaphylaxis
- key responsibility 8: preparing and implementing policies relating to prevention of cardiac arrest
- key responsibility 9: preparing and implementing a policy on resuscitation decisions, (for example, do not attempt cardiopulmonary resuscitation (DNACPR) decisions), and advance care planning (this is usually in collaboration with palliative care teams)
- key responsibility 10: quality improvement, action plans based on audits, for example, review of audit data using National Cardiac Arrest Audit data for benchmarking
- key responsibility 11: recording and reporting of patient safety incidents in relation to resuscitation
- key responsibility 12: the Resuscitation Committee is responsible for implementing operational policies governing cardiopulmonary resuscitation, practice and training
An annual audit report will provide assurance against each of the above key responsibility areas and will include relevant audit data.
11.1.8 Receipt of minutes and reports from
Completed resuscitation audits and any other relevant clinical audits undertaken.
11.1.9 reporting arrangements
Quality Committee for assurance in relation to the key responsibilities outlined in section 7 via an annual resuscitation report.
Safety and quality operational group.
The Executive Management team for any issues that require an urgent executive operational response.
Involvement of a designated non-executive director will have oversight of, and will sit as part of, the Resuscitation Committee.
11.1.10 Date
Each year.
11.1.11 Review date
Each year.
11.1.12 Document owner or responsibility for review (lead director)
Executive medical director.
11.2 Appendix B the deteriorating patient
Refer to appendix B: the deteriorating patient (staff access only).
11.2.1 Appendix B1 new head injury flow chart
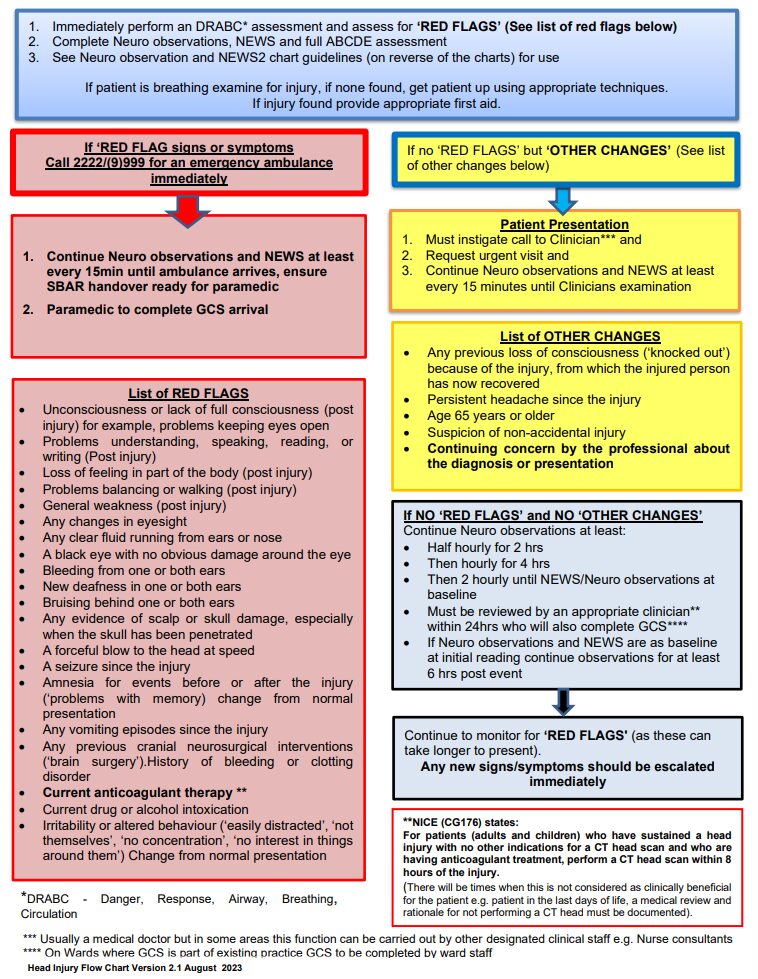
- Immediately perform a danger, response, airway, breathing, circulation (DRABC) assessment and assess for red flags (see list of red flags below).
- Complete neuro observations, NEWS and full airway, breathing, circulation, disability, exposure (ABCDE) assessment.
- See neuro observation and NEWS2 chart guidelines (on reverse of the charts) for use.
If patient is breathing examine for injury, if none found, get patient up using appropriate techniques.
If injury found provide appropriate first aid.
11.2.1.1 If red flag signs or symptoms
If red flags signs or symptoms call 2222 or (9)999 for an emergency ambulance immediately.
- Continue neuro observations and NEWS at least every 15 minutes until ambulance arrives, ensure a situation, background, assessment and recommendation (SBAR) handover ready for paramedic.
- Paramedic to complete GCS arrival.
11.2.1.1.1 List of red flags
- Unconsciousness or lack of full consciousness (post injury) for example, problems keeping eyes open.
- Problems understanding, speaking, reading, or writing (post injury).
- Loss of feeling in part of the body (post injury).
- Problems balancing or walking (post injury).
- General weakness (post injury).
- Any changes in eyesight.
- Any clear fluid running from ears or nose.
- A black eye with no obvious damage around the eye.
- Bleeding from one or both ears.
- New deafness in one or both ears.
- Bruising behind one or both ears.
- Any evidence of scalp or skull damage, especially when the skull has been penetrated.
- A forceful blow to the head at speed.
- A seizure since the injury.
- Amnesia for events before or after the injury (problems with memory) change from normal presentation.
- Any vomiting episodes since the injury.
- Any previous cranial neurosurgical interventions (brain surgery), history of bleeding or clotting disorder.
- Current anticoagulant therapy (NICE (CG176) states for patients (adults and children) who have sustained a head injury with no other indications for a computerised tomography (CT) head scan and who are having anticoagulant treatment, perform a CT head scan within 8 hours of the injury (there will be times when this is not considered as clinically beneficial for the patient, for example, patient in the last days of life, a medical review and rationale for not performing a CT head must be documented)).
- Current drug or alcohol intoxication.
- Irritability or altered behaviour (easily distracted, not themselves, no concentration, no interest in things around them) change from normal presentation.
11.2.1.2 If no red flags but other changes
If no red flags but other changes (see list of other changes below).
11.2.1.2.1 Patient presentation
- Must instigate call to clinician (usually a medical doctor but in some areas this function can be carried out by other designated clinical staff, for example, nurse consultants).
- Request urgent visit.
- Continue neuro observations and NEWS at least every 15 minutes until clinicians examination.
11.2.1.2.2 List of other changes
- Any previous loss of consciousness (knocked out) because of the injury, from which the injured person has now recovered.
- Persistent headache since the injury.
- Age 65 years or older.
- Suspicion of non-accidental injury.
- Continuing concern by the professional about the diagnosis or presentation.
11.2.1.2.3 If no red flags and no other changes
Continue neuro observations at least:
- half hourly for 2 hrs
- then hourly for 4 hrs
- then 2 hourly until NEWS or neuro observations at baseline
- must be reviewed by an appropriate clinician (NICE (CG176) states for patients (adults and children) who have sustained a head injury with no other indications for a computerised tomography (CT) head scan and who are having anticoagulant treatment, perform a CT head scan within 8 hours of the injury (there will be times when this is not considered as clinically beneficial for the patient, for example, patient in the last days of life, a medical review and rationale for not performing a CT head must be documented))
- within 24 hours who will also complete Glasgow Coma Scale (GCS)
on wards where GCS is part of existing practice GCS to be completed by ward staff - if neuro observations and NEWS are as baseline at initial reading continue observations for at least 6 hours post event
Continue to monitor for red flags (as these can take longer to present).
Any new signs or symptoms should be escalated immediately.
11.2.2 Appendix B2 ligature flow chart
Refer to appendix B2: ligature flow chart (staff access only).
11.2.3 Appendix B3 normal parameter exception care plan
Refer to appendix B3: normal parameter exception care plan (staff access only).
11.3 Appendix C emergency drugs
Refer to appendix C: emergency drugs (staff access only).
11.4 Appendix D emergency equipment
Refer to appendix D: emergency equipment (staff access only).
11.4.1 Appendix D1 equipment checklist
Refer to appendix D1: grab bag checklist (staff access only).
11.4.2 Appendix D2 equipment checklist
Refer to appendix D2: equipment checklist (staff access only).
11.5 Appendix E cardiac arrest report form
Refer to appendix E: cardiac arrest report form (staff access only).
11.6 Appendix F young people aged 16 and 17 years special considerations
Some special considerations apply where patients are aged 16 or 17 years.
11.6.1 Current practice relating to young persons
The Association for Children’s Palliative Care (2004) recommends that every young person with a life limiting condition should be helped, with their family, to decide on an end of life or palliative care plan.
Within the trust, the large majority of children (16 to 18 years) needing palliative care are under specialists in Sheffield.
11.6.2 Who should or could initiate discussion, and when?
It can be appropriate for professionals looking after young people with life limiting or life threatening conditions to initiate discussion about end of life planning well before the young person is terminally ill. It may also be appropriate to begin discussions if a young person has an acute illness or repeated illness as a result of which it becomes clearer to professionals and, or the parents that the young person is moving into a terminal phase of their illness, or that they are at an increased risk of a more sudden life threatening illness or event. Usually the most appropriate professional to initiate this discussion is the named paediatrician or palliative care practitioner.
If professionals initiate discussion, consideration should be given to the sensitive timing of this and further support for the family and young person may be necessary. Decision-making should not be forced on a young person or family. If a professional initiates a discussion about do not attempt cardio pulmonary resuscitation (DNACPR) and the young person or family indicate they do not wish to continue, their wishes should be respected, and the details recorded in the young person’s medical record.
Discussion may also be initiated by the young person or family at any time.
11.6.3 Who can make decisions?
The Department of Health (2009) state that:
“By virtue of section 8 of the Family Law Reform Act (1969), young people aged 16 and 17 are presumed to be capable of consenting to their own medical treatment. As for adults, consent will be valid only if it is given voluntarily by an appropriately informed young person capable of consenting to the particular intervention. However, unlike adults, the refusal of a competent person aged 16 to 17 may in certain circumstances be overridden by either a person with parental responsibility or a court.”
In exceptional circumstances it may be impossible for all concerned to reach a united decision regarding the best interest of the young person. If this cannot be resolved by the patient’s consultant, the consultant should request further advice from regional experts, trust medical director and trust legal services department.
To establish whether a young person aged 16 or 17 has the requisite capacity to consent to the proposed intervention, the same criteria should be used as for adults. If a young person lacks capacity to consent because of an impairment of, or a disturbance in the functioning of, the mind or brain then the Mental Capacity Act (2005) will apply in the same way as it does to those who are 18 and over (Department of Health (2009)).
Where a young person lacks capacity to decide, a person with parental responsibility for the young person may make a DNACPR decision where they consider that to be in the young person’s best interests.
If a 16 or 17 year-old is capable of making an informed decision then it is not legally necessary to obtain additional consent from a person with parental responsibility. It is, however, good practice to involve the young person’s family in the decision-making process, unless the young person specifically wishes to exclude them, if the young person consents to their information being shared.
If a young person decides that he or she does not wish to be resuscitated and that the family should not be involved with or informed about the decision this must be urgently referred to the trust medical director and legal services department.
11.6.4 What is, and who has, parental responsibility?
Parental responsibility is defined by section 3 of the Children Act (1989) as:
“All rights, duties, powers, responsibilities and authority which by law a parent of a child has in relation to a child and his property.”
Parental responsibility is therefore concerned with bringing the child up, caring for him and making decisions about him, including the right to consent or withhold consent for medical treatment. Parental responsibility is relinquished on a young person’s eighteenth birthday.
The Children Act (1989) sets out persons who may have parental responsibility. These include:
- the child’s mother
- the child’s father, if he was married to the mother at the time of birth
- unmarried fathers, who can acquire parental responsibility in several different ways:
- for children born before 1 December 2003, unmarried fathers will have parental responsibility if they:
- marry the mother of their child or obtain a parental responsibility order from the court
- register a parental responsibility agreement with the court or by an application to court
- for children born after 1 December 2003, unmarried fathers will have parental responsibility if they:
- register the child’s birth jointly with the mother at the time of birth
- re-register the birth if they are the natural father
- marry the mother of their child or obtain a parental responsibility order from the court
- register with the court for parental responsibility
- the child’s legally appointed guardian
- a person in whose favour the court has made a residence order concerning the child
- a local authority designated in a care order in respect of the child
- a local authority or other authorised person who holds an emergency protection order in respect of the child.
- it should be noted that:
- if a child is in local authority care parents can share parent responsibility with the local authority, this is lost if the child is adopted
- parental responsibility can also be restricted by a court order
- foster parents do not automatically have parental responsibility
- for children born before 1 December 2003, unmarried fathers will have parental responsibility if they:
11.6.5 Children in local authority care
Where a child is in the care of the local authority the child’s social worker must be involved in all of the discussions as well as parents, as the local authority shares parental responsibility with the parents. However, when a child is in voluntary care (section 20, Children Act (1989)) the parents retain full parental responsibility.
11.6.5.1 What happens when a young person and a person with parental responsibility disagree about a do not attempt cardiopulmonary resuscitation decision?
Decision-making with young people may be a matter of negotiation between the child, those with parental responsibility and clinicians. Inevitably there will be times when young people and those with parental responsibility for them do not agree about whether a do not attempt cardiopulmonary resuscitation (DNACPR) decision should be made.
If a young person is deemed to have the capacity to make a DNACPR decision (or believes he or she has capacity to make a decision?) and there is disagreement between the patient and those with parental responsibility despite attempts to reach agreement, legal advice should be sought.
What happens when medical staff and a young person or persons with parental responsibility disagree about a DNACPR decision?
Where medical staff are strongly of the opinion that cardiopulmonary resuscitation should not be attempted but the young person or people with parental responsibility disagree, or vice versa, a legal opinion should be sought.
11.6.6 Safeguarding issues
Where there is doubt about whether a person with parental responsibility is acting in the interest of the young person, then local safeguarding children board procedures must be instigated.
11.6.7 Education establishments
Potentially a young person may wish to continue at school with an agreed do not attempt cardiopulmonary resuscitation (DNACPR) decision in place. This can potentially cause anxieties for both the family and staff supporting that young person. Advice can be sought from a palliative care practitioner in dealing with those anxieties and what measures can be put in place to support the child and family during this period.
11.6.8 Interface with the child death overview process
Each safeguarding board has a designated paediatrician for all unexpected child deaths who are supported by a Rapid Response team. All deaths of a person under 18 years of age must be reported to the rapid response professional in the local area, who will notify the child death overview panel of the local safeguarding children board in accordance with the statutory guidance in chapter 7, Working Together to Safeguard Children 2010. Do not attempt cardiopulmonary resuscitation (DNACPR) status must be reported at this time. The rapid response team contact details can be found on the local safeguarding children’s board website.
11.7 Appendix G cardio-pulmonary resuscitation decision-making framework
- Is cardiac or respiratory arrest a clear possibility?
- No, it is not necessary to discuss cardiopulmonary resuscitation with the patient unless they express a wish to discuss it.
- Yes, is there a realistic change that cardiopulmonary resuscitation could be successful?
- No, if a do not attempt cardiopulmonary resuscitation (DNACPR) decision is made on clear clinical grounds that cardiopulmonary resuscitation would not be successful there should be a presumption in favour of informing the patient of the decision and explaining the reason for it (see section 5). Subject to appropriate respect for confidentiality those close to the patient should also be informed and offered an explanation. Where the patient lacks capacity and has a welfare attorney or court-appointed deputy or guardian, this representative should be informed of the decision not to attempt cardiopulmonary resuscitation and the reasons for it as part of the ongoing discussion about the patient’s re (see section 5). If the decision is not accepted by the patient, their representative or those close to them, a second opinion should be offered.
- Yes, does the patient lack capacity and have an advance decision specifically refusing cardiopulmonary resuscitation or have an appointed attorney, deputy or guardian?
- Yes, if a patient has made an advance decision refusing cardiopulmonary resuscitation, and the criteria for applicability and validity are met, this must be respected. If an attorney, deputy or guardian has been appointed they should be consulted (see sections 9.1 and 10).
- No, does the patient lack capacity?
- Yes, discussion with those close to the patient must be used to guide a decision in the patient’s best interests (see section 10). When the patient is a child or young person, those with parental responsibility should be involved in the decision where appropriate, unless the child objects (see section 11).
- No, is the patient willing to discuss his or her wishes regarding cardiopulmonary resuscitation?
- No, respect and document their wishes (see section 6.3). Discussion with those close to the patient may be used to guide a decision in the patient’s best interests, unless confidentiality restrictions prevent this.
- Yes, the patient must be involved in deciding whether cardiopulmonary resuscitation will be attempted in event of cardiorespiratory arrest.
- If cardiorespiratory arrest occurs in the absence of a recorded decision there should be an initial presumption in favour of attempting cardiopulmonary resuscitation.
- Anticipatory decisions about cardiopulmonary resuscitation are an important part of high-quality health care for people at risk of death or cardiorespiratory arrest.
- Decisions about cardiopulmonary resuscitation are sensitive and complex and should be undertaken by experienced members of the healthcare team with appropriate competence.
- Decision about cardiopulmonary resuscitation require sensitive and effective communication with patients and those close to patient.
- Decision about cardiopulmonary resuscitation must be documented fully and carefully.
- Decisions should be review with appropriate frequency and when circumstances change.
- Advice should be sought if there is uncertainty.
11.8 Appendix H do not attempt cardiopulmonary resuscitation form (WZT652)
Refer to appendix H: do not attempt cardiopulmonary resuscitation form (WZT652) (staff access only).
11.9 Appendix I do not attempt cardiopulmonary resuscitation communication sticker
Refer to appendix I: do not attempt cardiopulmonary resuscitation communication sticker (staff access only).
11.10 Appendix J What if my heart stops leaflet
This leaflet has been produced to help you understand what happens when your heart stops beating, how cardio-pulmonary resuscitation (CPR) can be used, and when it may not be helpful.
It may be upsetting to talk about resuscitation. This booklet tries to explain the issues as clearly and sensitively as possible.
You do not have to discuss resuscitation if you do not want to. However your health care team is available if you change your mind.
11.10.1 Why do people die?
It’s sad, but everybody dies.
Thinking about dying usually makes us sad, and perhaps a bit frightened.
It’s not something we like to think about, but talking with your family or with your doctor, and making plans for that time, can make things as easy as possible for you and those close to you.
Death might be due to an accident, or a sudden event, but most people die from serious illnesses which they have had for many months or even years.
11.10.2 What happens when my heart stops beating?
When you die your heart stops beating.
No blood gets pumped round your body, so very quickly the rest of your body stops working.
Your kidneys, your liver, your lungs all stop working.
Your brain will stop working about three minutes after your heart stops beating.
11.10.3 What is cardiopulmonary resuscitation?
If your heart stops beating it may be possible to start it beating again.
Attempts to restart your heart will include pressing down firmly on your chest again and again, and breathing for you.
This is called cardiopulmonary resuscitation (CPR).
Ambulance or hospital staff might use a machine to give your heart an electric shock to make it start working again.
They may put a tube down your windpipe to help you breathe, or give you drugs to help your heart start.
11.10.4 Do patients fully recover after cardiopulmonary resuscitation?
Each person has a different chance of cardiopulmonary resuscitation (CPR) working. Only about 2 out of 10 patients who have cardiopulmonary resuscitation survive and go home from hospital; survival is less likely in people with lots of health problems.
Even if cardiopulmonary resuscitation starts the heart again, patients usually need more treatment, often in an intensive care unit. Some patients never get fully better and suffer from mental or physical disabilities.
The decision to attempt cardiopulmonary resuscitation has nothing to do with how old you are or your abilities. It is about whether the treatment will help you.
Your doctor is the best person to decide if cardiopulmonary resuscitation is likely to help.
Cardiopulmonary resuscitation will not be attempted if it will only start your heart and breathing for a short time, or if it would prolong your suffering.
11.10.5 Will someone discuss cardiopulmonary resuscitation with me?
You might want to talk about what happens when you die, or you might have questions about cardiopulmonary resuscitation. It might be that because you have lots of health problems, cardiopulmonary resuscitation cannot help, and the health care team will decide not to attempt it when your heart stops. This is a do not attempt cardiopulmonary resuscitation (DNACPR) decision.
You have a right to be told if a DNACPR decision has been made, unless telling you would be harmful.
11.10.6 What if I don’t want to or am unable to talk about this myself?
You can appoint someone to have power of attorney for your health. This person is then allowed to speak on your behalf when you can’t do this yourself. If you cannot talk for yourself or don’t wish to, then the health care professionals in charge of your care will decide what treatment is best for you (this is a best interests decision). Wherever possible they will discuss this with those close to you.
11.10.7 What if I want cardiopulmonary resuscitation to be attempted?
Health care professionals will not refuse your wish for cardiopulmonary resuscitation (CPR) if it will be of benefit to you.
However, you cannot insist on having a treatment that will not work. Health care professionals will not offer treatment that will be degrading or cause harm.
If there is any doubt that cardiopulmonary resuscitation would work, the health care team can arrange a second opinion if you would like one.
If cardiopulmonary resuscitation might work, but it is likely to leave you severely ill or disabled, your opinion about whether the chances are worth taking is very important.
The health care team must and will listen to you.
11.10.8 What if I know I don’t want to be resuscitated?
If you don’t want cardiopulmonary resuscitation, you can refuse it, and your health care team must respect your wishes. You can talk to your doctor or nurse about this.
Your doctor or nurse can give you advice on making a legally binding advance decision to refuse treatment.
11.10.9 If it is decided cardiopulmonary resuscitation will not be attempted, what will happen next?
If you do not want cardiopulmonary resuscitation (CPR), or if your doctor decides that it will not work for you, a do not attempt cardiopulmonary resuscitation (DNACPR) form will be completed and discussed with you.
It tells everyone who looks after you that this decision has been made.
There is only one copy of the form which will be needed if you are admitted to hospice or hospital, or if you travel by ambulance. At home, it needs to be kept safe so that healthcare professionals can see it if needed.
11.10.10 What happens if my situation changes?
Your do not attempt cardiopulmonary resuscitation (DNACPR) form will state when the decision should be reviewed. If your health condition changes, the decision can be reviewed.
Your health care team will be happy to discuss any changes with you.
11.10.11 Can I see what is written about me?
You have a legal right to see what is written about you and can ask to do so.
If you do not understand what is written, your health care team will explain it to you.
11.10.12 What about other treatments?
If doctors decide not to attempt cardiopulmonary resuscitation, this will not affect any of your other treatment.
You will still receive the best care and medicines for your condition.
11.10.13 Who else can I talk to about this?
If you or your family do not think that you have had a chance to talk about this properly, please talk to a nurse or doctor looking after you.
If you don’t want to talk about it at all, that’s fine too.
There are people to listen if and when you do:
- your family, friends and carers
- a hospital chaplain, or someone from your own faith community
- an advocacy service
- community nursing teams
- palliative care teams
- your GP
- your district nurse
This leaflet has been adapted from an original collaboration between The Bradford and Airedale Palliative Care Managed Clinical Network for People with Learning Disabilities and Bradford Taking Media’s Access to Information for Minorities (AIM) Project.
The Yorkshire and Humber DNACPR Regional Working Group gratefully acknowledges the work of these groups.
11.10.14 References and further reading
11.10.14.1 The Bradford and Airedale palliative care managed clinical network for people with learning disabilities
Phone
11.10.14.2 Bradford Talking media
-
Address
11 to 12 Eldon Place
Bradford
BD1 3AZ -
Phone
11.10.15 Document control
Decisions relating to cardiopulmonary resuscitation, Royal College of Nursing, Resuscitation Council (UK), British Medical Association 3rd edition 2014 Deciding right, your life your choice. NHS England Northern Clinical Networks and Senate, April 2014.
11.11 Appendix K where to document the do not attempt cardio-pulmonary resuscitation decision in the electronic records
- Search for DNACPR in templates or locate RDaSH DNACPR in the left-hand clinical tree under corporate templates.

- Right click on RDaSH DNACPR.
- Click again on RDaSH DNACPR.
- The green information box will come up.

- Click the grey DNACPR tab at the top.
- This page gives a guide to DNACPR. The grey tab goes to the page to be completed, see next page.

- Tick the relevant boxes.
- Select the correct action from the drop-down menu, for example, not for attempted cardiopulmonary resuscitation.
- Write the details of the conversation with the patient or those closest to them, or the review on an existing document in the “detail of information” box.
- If having a review date, tick the box.
- If valid until the end of life, tick the box.
- Press OK and Save as normal.

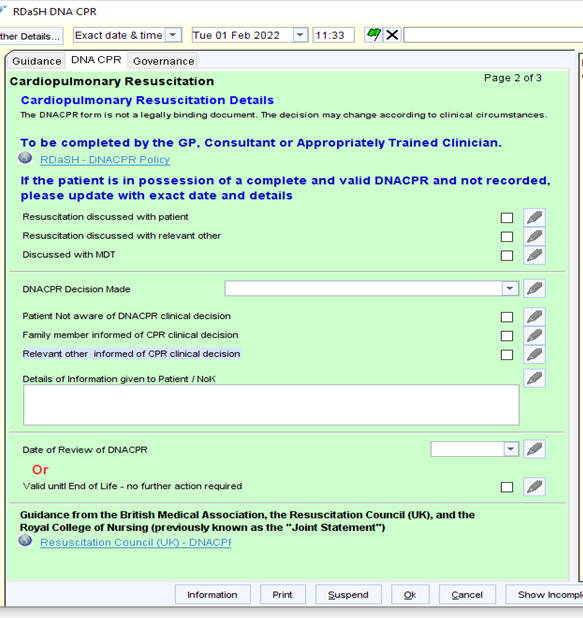
Document control
- Version: 2.
- Unique reference number: 629.
- Approved by: clinical effectiveness group.
- Date approved: 4 November 2025.
- Name of originator or author: resuscitation officer.
- Name of responsible committee or individual: chief nurse.
- Date issued: 24 December 2025.
- Review date: November 2028.
Page last reviewed: February 24, 2026
Next review due: February 24, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.