1 Introduction
Colleagues are our greatest asset, and our health and safety is important to us all.
There is need therefore, for colleagues to understand how to undertake safe manual handling practices, whilst the trust ensures legal responsibility to reduce the risk of injury. Poor manual handling techniques can result in musculoskeletal disorders, back pain and upper limb disorders. It is therefore essential that all colleagues receive appropriate manual handling training to enable them to carry out their duties safely and effectively.
The Manual Handling Operations Regulations (1992) (amended 2002) made under the Health and Safety at Work Act came into force on 1 January 1993 (European Directive 90/269/EEC). Under the regulations, employers must seek to avoid manual handling where possible. Where this is not possible, they are required to adopt an ergonomic approach to removing or reducing the risk of manual handling injuries through safe systems of work and a safe working environment.
2 Purpose
The purpose of this policy is to set out the trust’s arrangements associated with manual handling for:
- identifying and managing the risks associated with manual handling
- ensuring the delivery of effective manual handling training to all colleagues (not including Nation Health Service professionals (NHSP)), including the safe use of mechanical equipment in order to reduce the risks associated with manual handling
- recognising that safe methods of manual handling have considerable benefits for patients, including increased independence and personal safety
3 Scope
This policy applies to all colleagues who are employed by the trust, agency colleagues, students and volunteers (object handling only) who carry out manual handling activities, regardless of their location and covers the manual handling and lifting all objects and patients.
4 Responsibilities, accountabilities and duties
4.1 Chief executive
The chief executive as accountable officer of the trust has overall accountability for ensuring the trust meets statutory requirements. The responsibility for the management of manual handling is devolved to directors, managers, heads of department and to all trust colleagues.
4.2 The board of directors, deputy care group directors, corporate heads of service and managers
The board of directors, deputy heads of service, corporate heads of service and managers are responsible for ensuring that the trust consistently follows the principles of good governance applicable to NHS organisations. This includes the development of systems and processes to reduce the risk associated with manual handling. Their duties include and are not limited to:
- be responsible for ensuring this policy is publicised and implemented
- seek advice from the Manual Handling team where new services or service models are developed, or where new systems and tasks are introduced, in order that workplace planning and design regarding the elimination of manual handling hazards can be considered at an early stage
- make available adequate resources to meet the needs outlined within this policy
- maintain an up-to-date inventory of medical devices, including moving and handling equipment, accessories, servicing schedules, training needs, and maintenance records in line with the medical devices management policy. Ensure all manual handling equipment is regularly inspected, serviced, and maintained per the Lifting Operations and Lifting Equipment Regulations (LOLER) 1998 and Provision and Use of Work Equipment Regulations (PUWER) 1998 regulations
- appoint colleagues as manual handling key trainers and collaborate with them to identify, assess, and reduce risk from hazardous manual handling tasks
- monitor and review manual handling risk assessments when there is a reason to suppose that they are no longer valid due to accidents, changes in working conditions, personnel involved or a significant change in the manual handling operations affecting the nature of the task or the load
- clearly identify manual handling requirements of each job role when recruiting colleagues so that appropriate occupational health assessment can be undertaken as part of pre-employment health screening
- make reasonable adjustments for any known health problems or pregnancy which might have a bearing on an existing employee’s ability to carry out manual handling operations in safety
- refer to occupational health if there is reason to suspect that an individual’s health might increase the risk of injury from manual handling operations
- maintain records of incidents and ill-health issues related to manual handling operations and investigate the circumstances of the incident
- refer to the trusts fast track physiotherapy service as appropriate to maximise colleague recovery
4.3 Health and safety lead
Duties of the health and safety lead include but are not limited to:
- monitor the incidence and severity of all manual handling incidents throughout the trust and report on these to the health, safety and security forum
- liaise with the Manual Handling team in the investigation of manual handling incidents, analysis of causation and development of remedial action where appropriate
4.4 Health, safety and security forum
The purpose of the health, safety and security forum is to monitor and promote effective health and safety measures at work (HASAWA) 1974, section 2(7), through communication and collaboration between the trust and its employees on health and safety matters. A member of the Manual Handling team attends health, safety and security forum.
4.5 Manual Handling team
Duties of the Manual Handling team include and are not limited to:
- develop, implement and monitor safe systems of manual handling throughout the trust
- develop a trust wide action plan based on risk assessments and review this on an annual basis
- provide manual handling training for new starters as part of the trust corporate induction
- train the manual handling key trainers in both object and patient handling as appropriate and update them on an annual basis
- provide ongoing support and supervision to the manual handling key trainers
- be available as a source of expert, specialist advice to managers, colleagues and manual handling key trainers in the workplace
- maintain an up-to-date list of manual handling key trainers and accurate training records for monitoring or inspection purposes
- assist managers to undertake manual handling risk assessments and training needs analysis where new services or service models are developed, or where new systems and tasks are introduced
- monitor and advise on the sufficiency of the model of manual handling training
- following referral by a manager, conduct an assessment and provide advice in relation to manual handling in the workplace in order to assist a staff member’s return to work
- investigate manual handling incidents as requested by managers
- be involved in the assessment, trial and training associated with the implementation of new equipment to reduce manual handling risks
- provide advice to managers regarding pregnancy risk assessments in line with trust policy
- maintain a network of links with specialist advisors such as tissue viability, infection control and health and safety lead
- maintain records of all assessments and advice given
4.6 Manual handling key trainers
Duties of manual handling key trainers include and are not limited to:
- act as champions for safer manual handling operations, promoting trust policy and best practice
- work closely with managers to identify and risk assess manual handling tasks and to enable the most appropriate risk reduction measures to be developed and used
- train colleagues in up-to-date manual handling techniques, systems and legislation on a maximum ratio of 1 trainer to 6 colleagues
- provide the Manual Handling team with records of all training delivered
- attend an annual update provided by the Manual Handling team
- liaise with the Manual Handling team on an ongoing basis regarding manual handling issues in their teams or service areas
4.7 All colleagues
Duties of all trust colleagues include:
- taking reasonable care of their health and that of others whose safety may be affected by their activities when involved in manual handling operations
- cooperate with managers on risk assessments, follow safe systems and use provided equipment, report defects promptly, faulty equipment must be withdrawn from us and clearly labelled
- participating in statutory manual handling training and update training, two yearly for clinical colleagues and three yearly for non-clinical colleagues
- reporting pregnancy or any medical conditions which may affect their ability to handle loads safely to their manager
- reporting any change in working conditions, personnel involved in manual handling risks or a significant change in the nature of the task or the load, which may necessitate a review of the risk assessment
- maintaining records of risk assessments for dissemination to relevant colleagues
- wearing suitable work clothing and footwear for manual handling, see uniform and dress code policy
5 Procedure
The trust is committed to the implementation of a safer manual handling policy based on the following components:
5.1 Arrangements for access to appropriate specialist advice
Advice is provided by the trust’s Manual Handling team (staff access only) who can be contacted by phone or email:
The team delivers the trust’s manual handling training programme and when required, will seek the provision of additional external advice or equipment, for example, a piece of specialist equipment.
5.2 Techniques to be used in the moving and handling of patients and objects, including the use of appropriate equipment
5.2.1 Object handling
Object handling is taught according to the manual handling operations regulations approved code of practice which promote conditioning exercises, off-set base and a low centre of gravity.
Guidance continues to be sought from the Health and Safety Executive (HSE), The national back exchange and the Doncaster healthcare community manual handling passport.
Agile workers or hybrid workers can access extra support or guidance by clicking on this toolbox (staff access only).
5.2.2 Load handling
Apply a minimal lifting, individualised approach to load handling, guided by risk assessment. Use mechanical aids wherever possible. Reduce injury risk through strategic planning and workplace design to eliminate hazards early.
5.2.3 Patient handling
Manual handling of patients may be necessary but must be guided by duty of care and balanced decision-making. Manual lifting of adults should be avoided except in exceptional or life-threatening situations. Colleagues must not be expected to lift manually where safety is compromised; hoist or equivalent handling equipment must be used. The trust acknowledges this.
Colleagues attending manual handling training will receive knowledge and practical skill training on safer practices for both the patient and handler.
Colleagues who are unsure or concerned about any techniques currently being practiced should seek advice from a manual handling key trainer or the Manual Handling team.
If there are concerns that techniques used may constitute a safeguarding concern, then advice must be sought from the safeguarding team.
Each patient must be individually risk assessed, with active involvement in decision-making. Rehabilitation and developmental needs, alongside safety for colleagues, carers, and patients, must be considered. Manual handling may be used if it aligns with safer handling principles. In complex cases, seek guidance from a manual handling key trainer or team.
Risk assessments and manual handling action plans are filed in the patient record, SystmOne and shared with the colleague’s team. These should be reviewed at appropriate intervals or when circumstances change.
Note, for larger patients colleagues should refer to the care of the bariatric patient guidance.
5.2.3.1 Manual handling within the patient’s own home
Householders cannot be required by health and safety law to adapt their home or use equipment provided to reduce risks to visiting carers. However, with their co-operation, much can be done to eliminate or reduce the risks from manual handling, particularly by modifying the home environment to improve working postures of colleagues and carers. Organisations, however, do have a duty to colleagues working in patients’ homes.
Before discharge from hospital or following a home visit that has identified that a patient need has changed, colleagues must refer on to appropriate teams or services to address these needs.
Risk assessments should also be undertaken for the issue and delivery of equipment ensuring that safe systems of transportation are employed.
Where a risk assessment has been completed by a partner organisation or other health or social care practitioner, the content of the risk assessment and the recommendations will be recorded within the patient’s care record and shared. In addition, if colleagues notice that this information is missing, the patient needs have changed, or carers are failing to follow the risk assessment and plan, this should be escalated to the originator.
5.2.4 Rehabilitation handling of patients
Rehabilitation handling involves physical assistance as part of a planned therapeutic intervention. Risk must be mitigated through appropriate measures, including the use of standing and transfer aids, and additional colleagues where needed to support patient independence and mobility. Physiotherapists and occupational Therapists may perform handling as part of treatment, following safer handling principles and using equipment identified through risk assessment and moving and handling plans.
5.2.5 Workplace and environmental design
Consideration should be given to the suitability of the ergonomics for the task, such as the arrangement of doors and positioning of equipment. If necessary and possible, adjustments should be made to the environment to make the task safer.
5.2.6 Provision and use of equipment
Where risk assessments identify the need for manual handling equipment, authorised requisitioners must consult colleagues and the manual handling team to ensure suitability. Equipment should be demonstrated and trialled before purchase where possible.
5.3 How the trust risk assesses the moving and handling of patients and objects (further information is provided in appendices A and B)
5.3.1 Manual handling risk assessment
Two risk assessments are used: one for object and patient specific risks (appendix A), and one for patients (appendix B), with the latter available on SystmOne.
Assessments must consider task, individual capability, load and environment (TILE), and maybe generic or situation specific. Joint completion by qualified and unqualified colleagues is recommended to support balanced decisions and improve care plan compliance (Hignett et al. 2003).
Manual handling risk assessments will be recorded on the trust’s approved risk assessment documentation, which is in appendices A and B.
5.4 How action plans are developed as a result of risk assessments
- A trust wide action plan based on risk assessments is developed and reviewed as specified. This is also used to inform a review of manual handling training.
- For objects, action plans are written on the risk assessment forms.
- When reviewing the patient moving and handling assessment form colleagues should also consider the patient care plans and any other risk assessments to inform any changes to the moving and handling assessment form.
- For complex patients a personal handling profile is completed and added to the notes and stored electronically.
- Some risk assessments will lead to equipment adaptations or adjustments to reduce manual handling risks to the carer and or the patient. The proposed changes are likely to be more acceptable to the patient and their family if they have been fully involved in the assessment process and understand the purpose for which it has been carried out.
- However, even where there has been involvement in the assessment, a minority of people are reluctant to address the risks identified. This places the service provider in a difficult situation as they have a duty regarding colleague’s health and safety and the quality of care to the patient. It is not acceptable under health and safety legislation to allow unsafe work practices to continue.
In cases of disagreement, a balanced approach is essential to:
- protect colleagues and patients from unreasonable risk
- respect the patient’s preferences regarding mobility support
- promptly convene a meeting with the patient, family, and manager to review the risk assessment and care plan, ensuring a mutually agreed path forward
- where there is a difference of opinion, therefore, an urgent meeting with the patient, their family and the relevant manager should be held to discuss the risk assessment and care plan in order to agree a way forward
6 Training implications
The training needs analysis (TNA) for this policy can be found in the training needs analysis document which is part of the trust’s mandatory and statutory training policy located under the policy section of the trust website.
7 Monitoring arrangements
7.1 Duties
- How: report.
- Who by: Manual Handling team.
- Reported to: Health, safety and security forum.
- Frequency: annual.
7.2 Techniques to be used in the moving and handling of patients and objects including the use of appropriate equipment
- How: report by key trainer and individual referral for cases to the manual handling team and through incident reports and claims.
- Who by: Manual Handling team.
- Reported to: Health, Safety and Security Forum.
- Frequency: annual.
7.3 Arrangements for access to appropriate specialist advice
- How: report, email and referral system.
- Who by: Manual Handling team.
- Reported to: Health, Safety and Security Forum.
- Frequency: annual.
7.4 How the organisation risk assesses the moving and handling of patients and objects
- How: training and manual handling key trainer supervision.
- Who by: Manual Handling team.
- Reported to: Health, Safety and Security Forum.
- Frequency: annual.
7.5 How action plans are developed as a result of risk assessments
- How: report.
- Who by: Manual Handling team.
- Reported to: Health, Safety and Security Forum.
- Frequency: annual.
7.6 How action plans are followed up
- How: report by key trainer and individual referral or for cases to the Manual Handling team and through incident reports and claims.
- Who by: Manual Handling team.
- Reported to: Health, Safety and Security Forum.
- Frequency: 30 day follow up.
8 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
8.1 Privacy, dignity and respect
The NHS constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
As a consequence, the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
8.1.1 How this will be met
There are no additional requirements in relation to privacy, dignity and respect
8.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all colleagues working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
8.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005). (section 1) All assessments are carried out in collaboration with the patient. Should the patient not be able to express their views a best interest meeting is convened to look at the individualised patient’s manual handling needs.
9 Links to any associated documents
- Risk management framework
- Health and safety policy statement
- Health and safety policy
- Display screen equipment (DSE)
- Slips, trips and falls for staff and visitors, prevention and management policy
- Patient falls manual (prevention and management)
- Mandatory and statutory training policy
- Incident management policy
- Medical devices management policy
- Family leave policy
- Hoist and sling for safer patient use policy
- Care of the bariatric patient guidance
10 References
The health and safety executive (HSE) website provides further information and resources for managing the risks associated with manual handling health and safety executive.
- Manual Handling Operation Regulations 1992, updated 2002.
- Management of Health and Safety at Work Regulations, 1992.
- The Human Rights Act 1998.
- Provision and Use of Work Equipment Regulations, 1998 (PUWER).
- Lifting Operations and Lifting Equipment Regulations, 1998 (LOLER).
- Back Care (2011) The Guide to handling people (6th edition).
- Health and Safety at Work Act 1974.
- Hignett et al. (2003) Evidence Based Patient Handling.
11 Appendices
11.1 Appendix A patient moving and handling questionnaire user guide
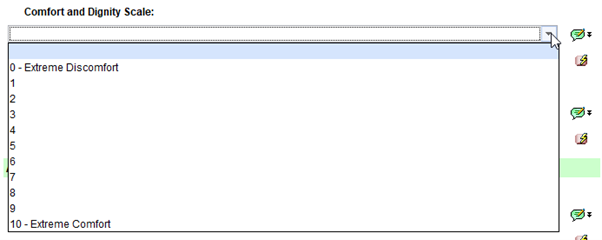
11.1.1 Comfort and dignity scale
Select between 0 and 10, 0 being extreme discomfort and 10 being extreme comfort.
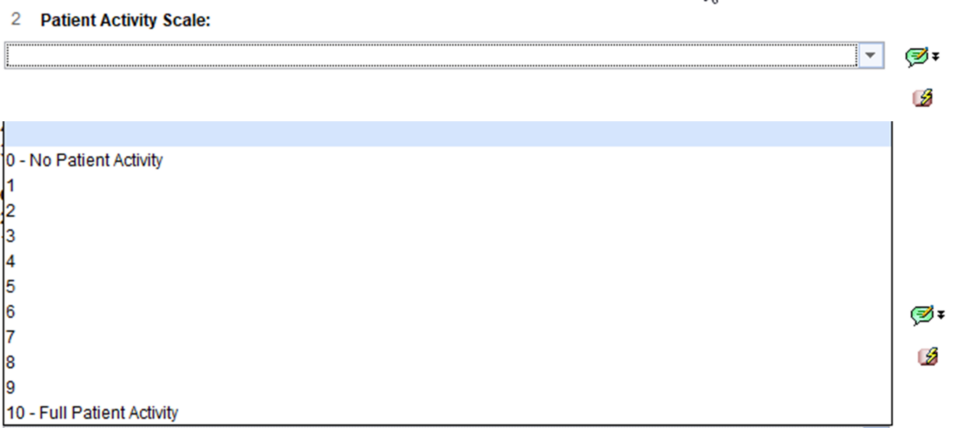
11.1.2 Patient activity scale
Select between 0 and 10, 0 being no patient activity and 10 being full patient activity.
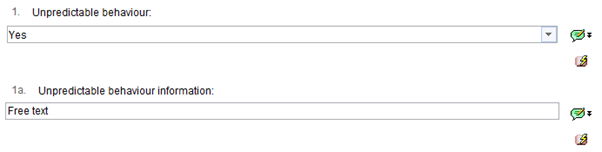
11.1.3 Section A, B, C further information
Sections A, B and C have a yes or no drop-down answer, if yes is selected a further information box will appear. These include unpredictable behaviour and information about unpredictable behaviour.
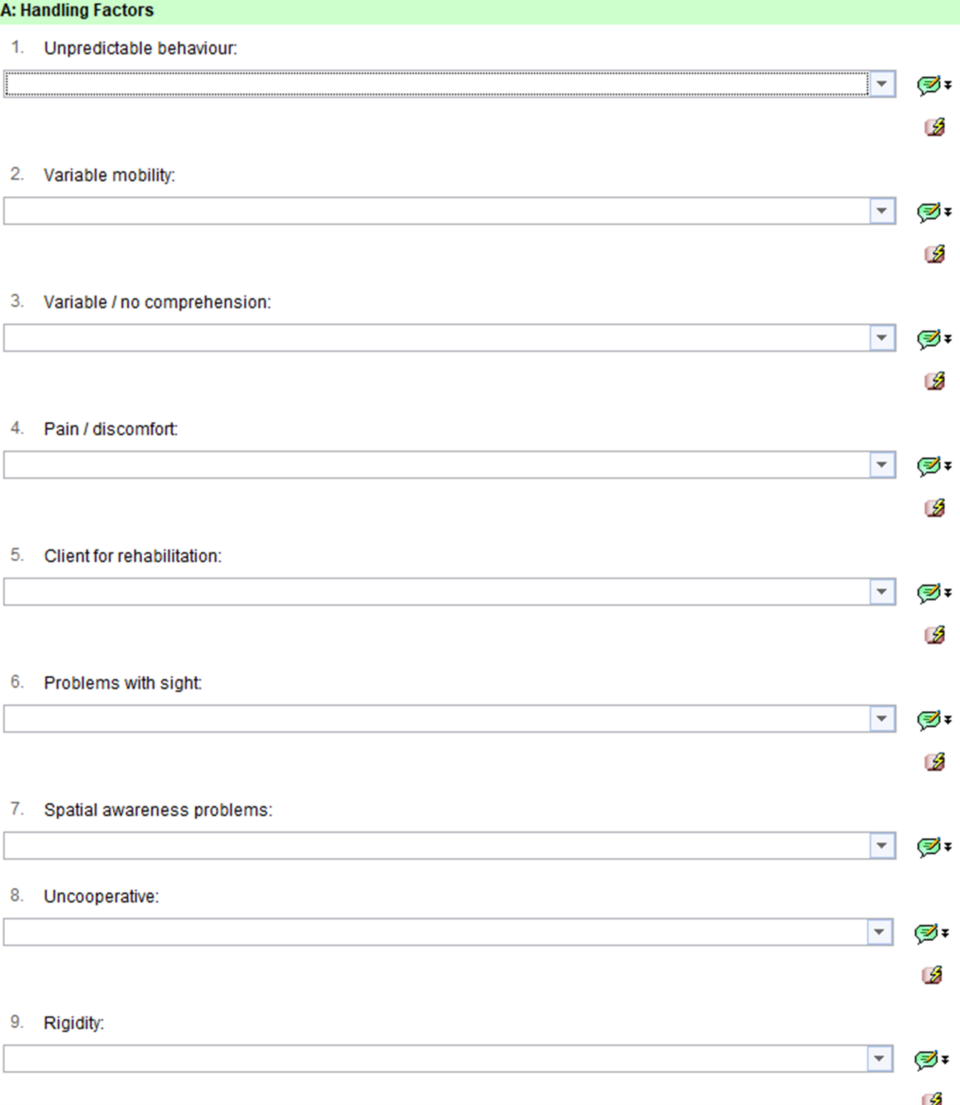
11.1.4 Section A, handling factors
Section A Handling Factors questions 1 to 9:
- unpredictable behaviour
- variable mobility
- variable or no comprehension
- pain or discomfort
- client for rehabilitation
- problems with sight
- spatial awareness problems
- uncooperative
- rigidity
11.1.4.1 Other, for example epilepsy, or medication
Free text box to enable other information to be entered.

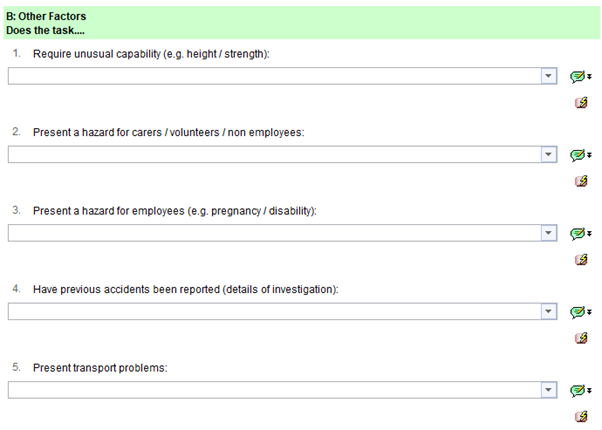
11.1.5 Section B, other factors
Other factors include:
- require unusual capability (for example, height or strength)
- present a hazard for carers, volunteers or non-employees
- present a hazard for employees (for example, pregnancy or disability)
- have previous accidents been reported (details of investigation)
- present transport problems
Complete with yes or no and further information option.
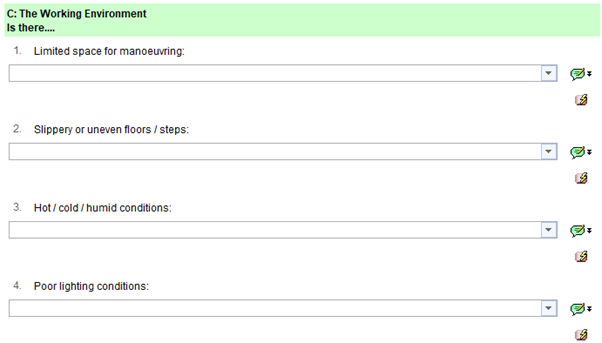
11.1.6 Section C, the working environment
Complete with yes or no and further information option.
Questions include:
- limited space for manoeuvring
- slippery or uneven floors or steps
- hot, cold or humid conditions
- poor lighting conditions
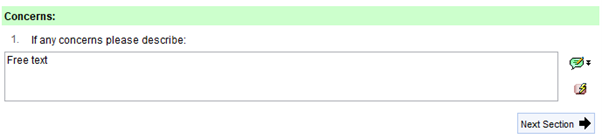
11.1.6.1 Concerns
Free text box to enable concerns information to be entered.
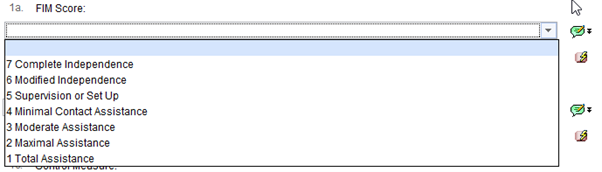
11.1.7 Method of manual handling
FIM Score (reference, The Guide to the Handling of People 6th Edition)
Independent, another person is not required for the activity (no helper)
- 7, complete independence
- 6, modified independence
Dependent, another person is required for verbal, gesture, physical prompt setup of environment. Or the task is not performed (requires help)
- 5, supervision or set up
- 4, minimal contact assistance
- 3, moderate assistance
Complete dependence, maximal or total assistance is required. Two people or more required or the task is not performed (requires 2 people to help)
- 2, maximal assistance
- 1, total assistance
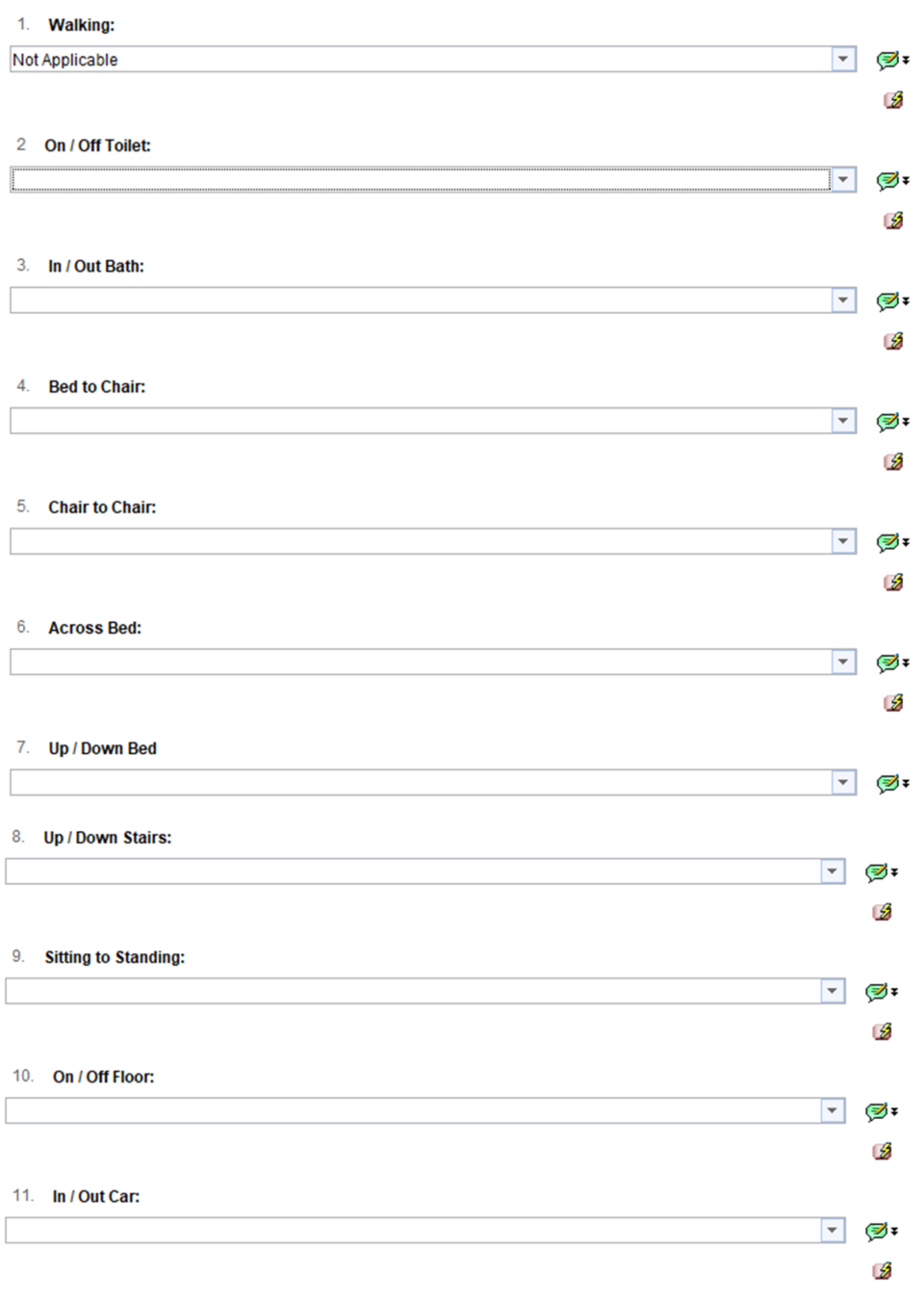
Questions 1 to 11 have a yes or no drop-down answer, if yes is selected further information is required to be filled in for FIM score, number of handlers and control measure.
11.1.7.1 Questions 1, 1a, 1b, and 1c
Questions include:
- walking
- FIM score
- number of handlers
- control measure
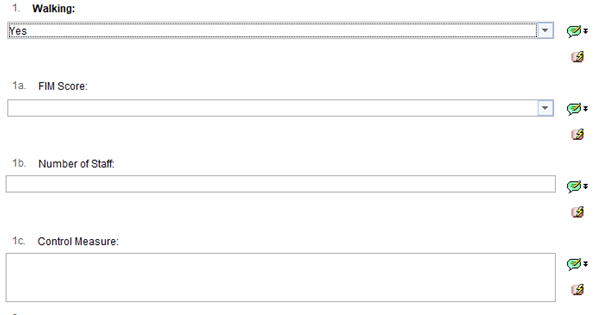
Question 1a, FIM score, select 1 to 7 depending on assistance or independence level.
Question 1b, number of handlers, free text box.
 Question 1c, control measure, free text box.
Question 1c, control measure, free text box.

11.1.7.2 Questions 1 to 11
Questions include:
- walking
- on or off toilet
- in or out bath
- bed to chair
- chair to chair
- across bed
- up or down bed
- up or down stairs
- sitting to standing
- on or off floor
- in or out car
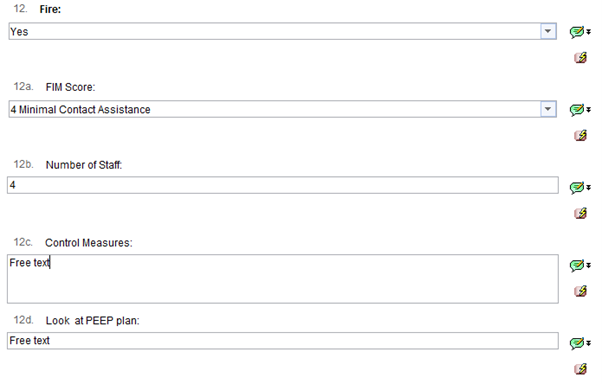
11.1.7.3 Questions 12, 12a, 12b, 12c, and 12d
Questions include:
- fire
- FIM score
- number of handlers
- control measures
- look at PEEP plan
Fire, if yes is selected an extra box populates this time to fill in, look at PEEP plan.
11.1.7.4 Question 13, other
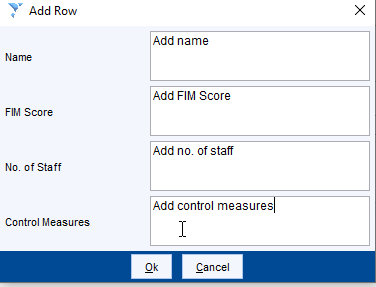
This is a table, select add row to add relevant information.
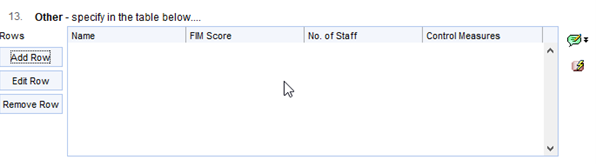
Fill in the information, name, FIM score, number of staff and control measures. Select “ok” once completed.
11.1.7.5 Question 14, training required
Last question, training required, this is a free text box to enable the relevant information to be added. Once everything is complete select finish.

11.1.8 Tips for using a questionnaire
Top left of the screen you will see the below buttons:
![]()
- Save for future editing, if you need to leave the questionnaire and come back to it, for example, have it checked, you can save the questionnaire for future editing. To complete the questionnaire, you must go back and save as final version.
- Save final version, a questionnaire must be completed as final version once finished.
- Use previous answers, this will allow you to pull through all previous answers used, the questionnaire should still be checked to make sure all the same answers are still relevant.
- Cancel, cancel out of the questionnaire, this will not save anything you have entered.
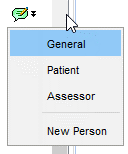
The green comments box allows you to add a comment, in general or from a specific person.
- Lightning bolt: allows you use the previous answer for that specific question.
- Green tick: page has been fully completed.
- Red cross: page has not been started.
- Green cross: page has been started but not fully completed.
![]()
11.2 Appendix B manual handling risk assessment form
Refer to appendix B: manual handling risk assessment form (staff access only).
11.3 Appendix C patient moving and handling assessment form
Refer to appendix C: patient moving and handling assessment form (staff access only).
11.4 Appendix D personal handling profile
Refer to appendix D: personal handling profile (staff access only).
Document control
- Version: 9.2.
- Unique reference number: 223.
- Approved by: Risk Management Group.
- Date approved: 6 January 2026.
- Name of originator or author: manual handling trainer.
- Name of responsible individual: director of people and organisational development.
- Date issued: 4 February 2026.
- Review date: 28 February 2029.
- Target audience: all colleagues.
Page last reviewed: February 04, 2026
Next review due: February 04, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem