2 Introduction
Rotherham, Doncaster and South Humber NHS Foundation Trust (RDaSH or the trust) aim to provide high quality, safe and effective services to all patients and recognises the importance of enabling effective continuity of care, particularly at times of transition when patients may be particularly vulnerable.
The transition from child to adult services can be a difficult time for young people. During this time there may be many other changes in a young person’s life, including changes from school to further pr higher education or employment; changes in self-identity and relationships; and changes which arise from the shift from childhood to adulthood, all of such can result in uncertainty, anxiety and stress.
As per National Institute for Health and Care Excellence (NICE) guidance 43 (NG43), it is important that any required transition process is managed sensitively and collaboratively to support both the continued engagement of the young person and their parents or carers and the safe and effective delivery of the required service. A young person’s experience of accessing, moving between or stepping down from services should be safe, well planned and prepared for, and they should feel supported and empowered to make decisions about their own health and social care needs.
Involving the young person and their parents or carers, ensuring collaborative working and effective communication between everyone involved is central to successful transition arrangements. These arrangements should involve preparing the young person for moving to adult services, the formal transfer of their care to a lead adult health professional and the subsequent support to establish them in the adult service. The process should be holistic and address the medical, psychosocial, educational and vocational needs of young people with chronic physical, mental, neurodevelopmental and medical conditions as they move from child-centred to adult-oriented healthcare systems.
Child and adolescent mental health services (CAMHS) and adult mental health services (AMHS) or learning disability (LD) services will work in partnership with young people and their parents or carers and with each other, sharing their expertise and resources to achieve smooth and effective transitional care arrangements for young people, and adequate support for their parents or carers.
3 Purpose
The purpose of this policy is to ensure a safe, effective and positive transition of care for those young people accessing child and adolescent mental health services (CAMHS) who, due to the ongoing nature of their health and, or mental health needs, will continue to require care and treatment from adult mental health or adult learning disability services.
This policy sets out the requirement for CAMHS, CAMHS intellectual disability (ID) teams and adult mental health services (AMHS) and adult learning disability (LD) teams, to ensure that their assessment and care planning systems interlink proactively and smoothly, in order that the experience of the young person is positive, and the transition arrangements and ongoing care provision is safe and effective.
4 Scope
Whilst this policy principally applies to young people up to the age of 18 who are under the care of child and adolescent mental health services (CAMHS) and CAMHS intellectual disability (19 for eating disorder services), practitioners should ensure that transition planning is developmentally appropriate and that it takes into account each young person’s capabilities, maturity, cognitive ability, psychological status, social and personal circumstances, caring responsibilities, communication needs, needs in respect of long-term conditions and hopes for the future.
This policy applies to all clinical colleagues working in the mental health directorate of the children’s care group, those working in adult mental health services and adult learning disability services.
For further information about responsibilities, accountabilities and duties of all employees, please see appendix A.
4.1 Safeguarding
Where there are complexities around safeguarding, practitioners are to liaise with safeguarding partners and to contact and consult with the trust Safeguarding team as appropriate.
4.2 Transitions and the Care Act (2014)
To be aware that section 58(1), Care Act (2014) states where it appears to a local authority that a child is likely to have needs for care and support after becoming 18, the authority must, if it is satisfied that it would be of significant benefit to the child to do so, assess:
- whether the child has needs for care and support and, if so, what those needs are
- whether the child is likely to have needs for care and support after becoming 18 and, if so, what those needs are likely to be
5 Procedure
5.1 Quick guide
5.1.1 Key point 1
All young people requiring transition into adult mental health services (AMHS) or adult learning disability services will be allocated a future key worker, lead professional or allocated worker from adult services once they reach 17 years and 6 months of age.
5.1.2 Key point 2
The young person, their parents or carers, their current child and adolescent mental health services (CAMHS), child and adolescent mental health services intellectual disabilities key worker, lead professional, allocated worker and their future adult, adult learning disability key worker, lead professional or allocated worker will meet to agree a transition plan.
5.1.3 Key point 3
Child and adolescent mental health services (CAMHS) or child and adolescent mental health services intellectual disabilities will continue to lead the care of the young person until transition is completed, and the young person is formally discharged from child and adolescent mental health services intellectual disability.
5.1.4 Key point 4
Where a referral is received into child and adolescent mental health services (CAMHS) or child and adolescent mental health services intellectual disabilities for a young person who is within 6 months of transition age, choice of service will be offered following review with adult services and consideration of age appropriateness or emotional maturity in line with ensuring that the trust is offering developmentally appropriate healthcare.
5.1.5 Key point 5
A transition tool should be used to help support this process; services may wish to consider the use of the Ready Steady Go tool (transition and patient empowerment innovation, education and research (TIER) network) to consider transition holistically, which may require input and support from external agencies.
5.2 General principles of transition
The transition process must be managed sensitively and collaboratively to support continued engagement of the young person and their parents or carers and safe and effective service delivery.
Commencing the transition process should be considered 6 months prior to service age limit, considering the clinical reasoning for requirement of ongoing treatment and intervention moving forwards for the young person.
In circumstances where treatment can be concluded within child and adolescent mental health services (CAMHS) but would potentially end beyond 18 years of age, CAMHS would be able to continue treating the young person to reduce the requirement to transfer care and therefore provide continuity for the young person.
Where a referral is received into CAMHS or CAMHS intellectual disabilities for a young person who is within 6 months of transition age, choice of service will be offered and age appropriateness or emotional maturity considered in line with ensuring developmentally appropriate healthcare.
Services for children and young people, and services for adults will benefit from having a good understanding of each other’s service provision and offer. Good knowledge of the service that a young person is being referred to or received from supports engagement with young people in the process, they are assisted to understand the service offer moving forwards and how this may be similar or different to current service provision.
To support effective joint working between services, regular attendance at each other’s team meetings is encouraged to share developments, explore any challenges or concerns and increase communications.
Joint working and care planning between CAMHS, CAMHS intellectual disability and adult mental health services or adult learning disability services identifies the transition process and who is responsible for which element of the transition plan and care plan delivery. Timely allocation of an identified future key worker, lead professional or allocated worker is imperative for a positive transition. See appendix A for an example of a transition care plan.
The majority of the Mental Capacity Act (2005) applies to young people aged 16 to 17 years who may lack capacity. All colleagues must therefore work within the provisions of the act and its Code of Practice (2007). See Mental Capacity Act (2005) policy and Deprivation of Liberty (DoL) policy.
Due consideration will be given to the content and wishes of any Advance Statement produced by the young person.
All discussion and decision-making should take place as far as possible with the involvement of the young person, their parents or carers and relevant workers of both child and adult services during the transition process.
A transition tool should be used to help support this process, services may wish to consider the use of the Ready Steady Go tool (Home: transition and patient empowerment innovation, education and research (TIER) network).
5.3 Transition from child and adolescent mental health services or child and adolescent mental health services intellectual disabilities to adult mental health services or adult learning disability services
The child and adolescent mental health services (CAMHS) key worker, lead professional or allocated worker will identify those young people known to their services who are age 17 years and 6 months, whose care will potentially need to transfer to adult services. For locality specific arrangements for transition to adult mental health services see appendices B to D, for CAMHS intellectual disabilities to adult learning disability service transition see appendix E.
Once agreement has been reached about which adult service will be appropriate for the young person to transition to, discussions will take place with the young person, their parents or carers and if possible, a peer support worker.
Adult mental health services and adult learning disability services will identify a key worker, lead professional or allocated worker who will liaise with the CAMHS, CAMHS intellectual disabilities key worker, lead professional or allocated worker. A joint transition meeting will take place, to include the young person and their parents or carers, and peer support worker if possible and in line with the wishes of the young person. The purpose of this meeting will be to discuss and agree with the young person and their parents or carers the components of, and responsibility for the transition plan and any ongoing needs identified in the young person’s care plan, including identification and management of any safety or risk issues.
A transition plan will be developed and recorded in collaboration with the young person to address the following issues:
- future care plan needs, and services offered within adult mental health services or adult learning disability services
- timescales for transition
- involvement of peer support worker
- communication and involvement of parents or carers
- discharge plans from CAMHS or CAMHS intellectual disabilities
- Wider transition needs which may involve external agency support
The responsibility for leading the transition arrangements will remain with CAMHS or CAMHS intellectual disabilities if the young person is accessing CAMHS or CAMHS intellectual disabilities at the time of being eligible for adult services. An initial transfer plan will be agreed between CAMHS or CAMHS intellectual disabilities and the key worker, lead professional or allocated worker from adult mental health services or adult learning disability services.
Both CAMHS or CAMHS intellectual disabilities and adult mental health services or adult learning disability services (as appropriate) will share equal responsibility for the delivery of care for the young person throughout the transition process and CAMHS or CAMHS intellectual disabilities will only discharge that duty of care at the end of the agreed transfer process.
Wherever possible, when significant mental health problems have already been identified, the treatment episode should continue until completion with CAMHS or CAMHS intellectual disabilities or until an appropriate transitional point is reached within the care plan.
A CAMHS or CAMHS intellectual disabilities discharge date will be agreed within the transition plan, and executed upon completion of the transfer, then formally recorded. The point of transfer should occur at relative stability wherever practicable and not be bound by rigid age thresholds.
Information relevant to the provision of effective care and treatment will be shared with the consent of the young person. Practitioners must take care to discuss clearly with parents or carers the changes in information sharing once their young person reaches the age of 18. Changes in information sharing may be instigated before the age of 18 years, if the young person is deemed able to give their direct consent. Careful and transparent conversations will support, and frame expectations enabling a smoother transfer and transition process. Only in exceptional circumstances will information be shared without a young person’s consent, that is, in line with local policies to ensure safe and effective service delivery. If over 16 and lacks capacity information can be shared in their best interests. If under 16 and not Gillick competent then consent can be given from a person with parental responsibility.
Transitional arrangements will be implemented at a pace with which the young person and their parents or carers are comfortable, and which promotes consistent quality, safety and continuity of care.
Where a young person has an education, health and care plan (EHCP) in place, this will inform and support the transition between services. education, health and care plans cover children and young people from 0 to 25 years of age, as part of the Children’s Act (2014) supporting access to education where a young person has additional needs.
5.4 New referrals to adult mental health services
For new referrals into the trust for young people aged 17 years and 6 months or over, consideration of services will be completed by CAMHS or CAMHS intellectual disabilities and adult mental health services or adult learning disability services (via the getting advice or Single point of Access team) or the specialist intellectual disability or learning disability teams. Consideration will be given to the preference of the young person and their parents or carers, the expected duration of intervention required and their current presenting needs.
5.5 Transition and joint working between child and adolescent mental health services and the early intervention in psychosis teams
For young people aged under 16 years, responsibility of care coordination will be led by the child and adolescent mental health services (CAMHS) key worker or lead professional or allocated worker, with close liaison with the Early Intervention in Psychosis team for additional support as necessary. Medical input will be provided by a child and adolescent psychiatrist with support from the early intervention in psychosis psychiatrist for those under 16 years of age.
For young people aged between 16 and 18 years, responsibility of care coordination will be led by the Early Intervention in Psychosis team, with any additional support and, or therapeutic interventions provided by CAMHS as required if beneficial for the young person and their family. Medical input will be provided by the Early Intervention in psychosis psychiatrist. See appendix H for further detail.
5.6 Transition and Joint working between child and adolescent mental health services and talking therapies
Young people from the age of 16 years can access the adult talking therapy services for their anxiety and depression. This pathway is not to replace services for those young people whose needs are best served within child and adolescent mental health services (CAMHS) or children’s services. It is instead for those young people 16 and over who can make a choice on whether they would like to access short-term talking therapy through an adult’s service. This pathway is also not intended to help control or manage CAMHS waiting list for treatment. Liaison meetings between CAMHS clinical leads and talking therapies clinical leads will occur regular to ensure the smooth transfer of patients. This pathway has agreed inclusion and exclusion criteria and flow charts (appendix G).
6 Training implications
No specific training for transition.
As a trust policy, all colleagues need to be aware of the key points that this policy covers. Colleagues can be made aware through:
- team meetings
- one to one supervision
- learning half day
- practice development days
- local induction
7 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
7.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, “not just clinically but in terms of dignity and respect”.
As a consequence, the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
7.1.1 How this will be met
This policy supports the development of personalised care planning for young people who are transitioning from child and adolescent mental health services to adult mental health and learning disability services.
7.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
7.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the Mental Capacity Act (2005) (section 1).
8 Links to any other associated documents
- Care programme approach (CPA) policy
- Safeguarding children policy
- Disengaging with services (children and young people and child and adolescent mental health services) policy
- Consent to care and treatment policy
- Mental Capacity Act (2005) policy
- Advance statements and advance decisions to refuse treatment
- Supervision policy
- Mandatory and statutory training policy
- Mental Capacity Act deprivation of liberty (DoL) policy
10 References
- National Institute for Health and Care Excellence (NICE) guidance 34 (NG34)
- Home: transition and patient empowerment innovation, education and research (TIER) network
11 Appendices
11.1 Appendix A Responsibilities, accountabilities and duties
11.1.1 The board of directors
The board of directors has responsibility for the implementation of this policy and the monitoring of compliance. This responsibility is delegated to the trust chief executive who will delegate lead strategic responsibility to a director.
11.1.2 Chief operating officer
As nominated strategic lead, the chief operating officer is responsible for:
- the implementation of all policies and procedures which are in place to meet the needs of patients
- monitoring adherences to this and other related policies
- adequate resources and training being available to the clinical teams
- monitoring colleague compliance with training as set out in the mandatory and statutory training policy and mandatory risk management training needs analysis matrix
- the development, implementation and monitoring of effective systems of supervision for clinical colleagues
11.1.3 Chief medical officer
The executive medical director is responsible for providing clinical leadership within the trust and for the provision of senior clinical advice to the board of directors. The executive medical director is responsible for resolving issues where there are differences of opinion, which cannot be resolved by the care group medical directors.
11.1.4 Chief nursing officer
The chief nursing officer has lead responsibility for clinical assurance within the trust, supported by the deputy chief nursing officer. They are responsible for supporting the implementation of this policy through, for example, clinical audit and mandatory risk management training.
11.1.5 Care group directors
Children’s, Doncaster mental health and learning disability, Rotherham, North Lincolnshire and talking therapies.
Care group directors are responsible for:
- the implementation of the policy across the specified care groups
- the ongoing review of the policy to keep it up-to-date with current best practice
- promoting collaborative working between services, in order that the needs of the patient remain at the centre of the process
- providing reports to the operational management group (OMG) on any issues associated with the implementation of the policy
- facilitating effective joint working with internal and external partners and stakeholders
- monitoring colleague compliance with the relevant mandatory risk management training as set out in the mandatory and statutory training policy and mandatory risk management training Needs analysis matrix
- the development, implementation and monitoring of effective systems of supervision for clinical colleagues within their care groups
11.1.6 Care group medical directors
Children’s, Doncaster mental health and learning disability, Rotherham, North Lincolnshire and talking therapies.
The supportive and facilitative role of the care group medical director is to provide advice to clinical colleagues within the care groups. The care group medical director may be asked to advise and, or provide a second opinion for patients with complex needs where there are professional differences of opinion between care groups.
11.1.7 Service managers
Child and adolescent mental health services, adult mental health services and adult learning disability services.
- Service managers are responsible for the implementation of the policy within their areas of responsibility.
- They are the next point of escalation in cases where there are differences of opinion between team manager or pathway lead and, or at pathway meetings.
- They will monitor and ensure that all relevant colleagues access the required mandatory risk management training as set out in the mandatory and statutory training policy and mandatory risk management training needs analysis matrix.
11.1.8 Team manager or pathway leads
Child and adolescent mental health services, adult mental health services and adult learning disability services.
- The team manager or pathway lead is responsible for identifying the number of colleagues, and the appropriate level of training required for those colleagues to deliver safe and effective services.
- The adult mental health services and adult learning disability services managers or pathway leads are responsible for ensuring appropriate allocation of transition cases to colleagues.
- The team manager or pathway lead is responsible for the provision and monitoring of supervision within their team in line with the clinical and management supervision policy for clinical colleagues.
- The child and adolescent mental health service team manager or pathway lead is responsible for ensuring that appropriate, relevant and up-to-date information is provided to the adult service which the young person is transferring to adult mental health services and adult learning disability services will identify a key worker for child and adolescent mental health service colleagues to liaise with in relation to identifying the relevant team to meet the ongoing needs of the young person and resolve any transition issues.
11.1.9 Community clinical colleagues
Child and adolescent mental health services, adult mental health services and adult learning disability services) key worker, lead professional or allocated worker.
- Working collaboratively with colleagues in child and adolescent mental health services or adult mental health services to ensure that the needs of the young person remain at the centre of the transition process. Implementing this policy and the guidance set out within the move to personalised care standard operating procedure.
- Implementing the disengaging with services (children and young people and child and adolescent mental health services) policy.
- Informing the appropriate team manager or pathway lead of any circumstances in which the implementation of this policy is compromised.
- Child and adolescent mental health services practitioners will provide up-to-date relevant clinical information to summarise current care and treatment needs of the young person, alongside future care needs as identified and agreed with the young person.
11.1.10 All clinical colleagues involved in the delivery of care to children, young people and adults
All clinical colleagues involved in the delivery of care to children, young people and adults, are responsible for alerting the key worker, lead professional or allocated worker of any concerns regarding quality, safety or effectiveness of care or if a child or young person has not attended an appointment or it is suspected that they are disengaging from services.
11.1.11 Peer support workers
Based within child and adolescent mental health services (CAMHS) or CAMHS intellectual disabilities.
Peer support workers help young people, their parents or carers and their CAMHS workers by supporting a young person’s transition to adult services or discharge from CAMHS as they approach 18 years old.
Through their own lived experiences, peer support workers are better able to understand a young person’s situation.
Peer support workers support the young person, by:
- building a relationship with them, using their own “lived experiences” to show a deeper understanding of their situation
- listening to the young person fully and helping them to explore their hopes and fears about the future.
- encouraging young people to take responsibility for themselves and their mental health
- helping young people to become more independent
- helping the young person to become familiar with adult services (location of services, people to know, et cetera)
- creating a plan to manage their health and wellbeing which they can implement with support from adult services
- supporting the young person, their parents or carers and their CAMHS worker to make their transition to adult services or discharge run smoothly
- peer support workers will work collaboratively with the key worker, lead professional or allocated worker to support the delivery of the transition plan and care plan
- alert the key worker, lead professional or allocated worker of any concerns regarding quality, safety or effectiveness of care, or if a child or young person has not attended an appointment or it is suspected that they are disengaging from services
11.2 Appendix B monitoring arrangements
11.2.1 Number of transitions taking place with a care plan in place
- How: quarterly report to commissioners.
- Who by: Performance team.
- Reported to: finance, performance and people meeting and local commissioners.
- Frequency: quarterly.
11.3 Appendix C example transition care plan
11.3.1 Summary of problem or need
Move from child and adolescent mental health services to adult mental health services for ongoing mental health interventions.
11.3.2 Goal, what do we want to achieve?
To transfer from child and adolescent mental health services to adult mental health services in a planned and supported way.
11.3.3 How will we know that we have achieved it?
I will be receiving support from a new adult mental health worker and engaged in treatment.
We will agree what I want to achieve from coming to the adult mental health services and how we are going to do this
11.3.4 Actions
- Meeting to be held between child and adolescent mental health services and adult mental health staff member.
- Meeting with me, my child and adolescent mental health services worker, my peer support worker and my Mum to discuss the new service and my needs.
- We will agree what I want to achieve from coming to the adult mental health services and how we are going to do this.
- My mum will also have the opportunity to talk about her worries about the change.
- The peer support worker will help me to get used to going to the new place for appointments and offer support.
11.3.5 Involvement, who will do what?
My child and adolescent mental health services worker will talk about the change in services.
The peer support worker will help with the practical things (going to the new venue, et cetera).
The adult mental health worker will work with me on a new care plan.
11.3.6 Timeframe, when will we aim to have this done by?
It is planned that the transition will have happened by my 18th birthday, but if this hasn’t occurred, we will review the timescales to when it feels right.
11.4 Appendix D child and adolescent mental health services to adult mental health services transition pathway
![]()
- Child and adolescent mental health services young person reaches 17 years and 6 months (18 years 6 months for eating disorders).
- Is there a need for continuing treatment that cannot realistically be completed in child and adolescent mental health services?
- No, work towards discharge from child and adolescent mental health services, taking into consideration wider transitional needs of the young person which may require liaison with external agencies. Discharge from child and adolescent mental health services.
- Yes, discussion with young person regarding onward referral to adult services. Contact made with adult mental health services to establish the most appropriate adult service.
- Referral criteria or checklist to include:
- summary
- risk (self or others)
- behaviour
- vulnerability or safeguarding
- Child and adolescent mental health services worker arranges to and attends team meeting of appropriate adult mental health services to discuss young person’s needs and identify appropriate key worker.
- Within 4 weeks of child and adolescent mental health services attending team meeting: meeting held between child and adolescent mental health services worker, identified adult mental health services worker, young person, parent or carer and peer support worker (as appropriate) for introductions, questions and answers and to develop agreed transition plan, including frequency of joint meetings during transition period.
- Transfer is complete and adult services take over care of the young person.
- Discharge from child and adolescent mental health services.
11.5 Appendix E Rotherham child and adolescent mental health services intellectual disability and adult learning disability transition process
- Transition’s cases from child and adolescent mental health services intellectual disability to adult learning disability services to begin from 17 and a half years of age. Cases between 17 and 17 and half if complex to begin early.
- Child and adolescent mental health services intellectual disability transition agenda to adult learning disability services document to be completed by child and adolescent mental health services intellectual disability transition coordinator.
- Microsoft Teams transition meeting every three months last Wednesday 2pm to 3pm.
- No transition cases or potential transitions to discuss, email rdash.rotherhamldadmin@nhs.net to cancel the meeting.
- Transition document to outline:
- name
- date of birth
- NHS number
- care coordinator
- other services or professionals involved
- risk: low, medium or high
- proposed pathway
- diagnosis
- identified needs or challenges
- pharmacological treatment plans
- Action points to be documented in section 4 action log via transition document by child and adolescent mental health services intellectual disability transition coordinator. Transition document with action points to be disseminated with adult learning disability service colleagues and child and adolescent mental health services care coordinator of cases.
- Cases that require prescribing input for attention deficit hyperactivity disorder (ADHD) treatment, to be completed via the adult service health form and emailed to rdash.rotherhamldreferrals@nhs.net.
- Adult service health referral form to be completed if agreed to do so at transition meeting.
- Psychometric questionnaires to be completed and sent with single access referral form:
- mGASS (if cases prescribed anti-psychotics only)
- easy read Glasgow
- depression and anxiety scale (treating depression or anxiety if patient can participate)
- Formulations, assessment reports, plans and psychiatry clinic letters to be sent with adult health service form. Up-to-date face risk, care plans, at the last transition step to be available via system one for adult learning disability service colleagues proposed pathway if for adult psychiatry only, respective child and adolescent mental health services intellectual disability prescriber to write directly to adult psychiatry with most up-to-date pharmacological treatment plan and the most up-to-date physical health monitoring information.
- Child and adolescent mental health services intellectual disability transition coordinator to document via child and adolescent mental health services intellectual disability launch pad discharge or transition or task the care coordinator to add information from health referral form and transition document.
- Referral accepted: joint transition to commence between care coordinators allocated from child and adolescent mental health services intellectual disability and adult learning disability service introduction, meetings, clinic appointments adult learning disability coordinator to be invited.
- Pharmacological treatment for depression or anxiety, adult learning disability psychiatrist to decide prior to the young person turning 18 to accept or signpost to GP for ongoing treatment (Melatonin to be accepted). Prescribing to be continued by child and adolescent mental health services intellectual disability until the first appointment with adult learning disability psychiatry.
- If identified no role for adult learning disability, adult learning disability service leaflet to be sent alongside discharge from child and adolescent mental health services intellectual disabilities to make young persons and carers aware of adult service support if required in the future.
11.6 Appendix F Doncaster child and adolescent mental health services intellectual disability and adult learning disability transition process
- Transition’s cases from child and adolescent mental health services intellectual disability to adult learning disability to begin from 17 and a half years of age. Cases between 17 and 17 and a half if complex to begin early.
- Child and adolescent mental health services intellectual disability transition agenda to adult learning disability services document to be completed by child and adolescent mental health services intellectual disability transition coordinator.
- Face to face Tickhill Road site 2 Jubilee Close or Microsoft Teams transition meeting every three months first Tuesday 9:30am to 10:30am.
- No transition cases or potential transitions to discuss to email rdash.adultldservices@nhs.net to cancel the meeting.
- Transition document to outline the following information:
- name
- date of birth
- NHS number
- care coordinator
- other services or professionals involved
- risk: low, medium or high
- proposed pathway
- diagnosis
- identified needs or challenges
- pharmacological treatment plans
- Action points to be documented in section 4 action log via transition document by child and adolescent mental health services intellectual disability transition coordinator. Transition document with action points to be disseminated with adult learning disability colleagues and child and adolescent mental health services care coordinator of cases.
- Cases that require prescribing input for attention deficit hyperactivity disorder (ADHD) treatment, Doncaster adult neurodevelopmental service (DANS) form to be completed and emailed to rdash.neurodiverse-team@nhs.net.
- Single access referral form (SARF) to be completed if agreed to do so at transition meeting.
- Psychometric questionnaires to be completed and sent with single access referral form:
- mGASS (if cases prescribed anti-psychotics only)
- easy read Glasgow
- depression and anxiety scale (treating depression or anxiety if patient can participate)
- Formulations, assessment reports, plans and psychiatry clinic letters to be sent with single access referral form. Up-to-date face risk, care plans, at the last transition step to be available via system one for adult learning disability colleagues. Proposed pathway if for adult psychiatry only, respective child and adolescent mental health services intellectual disability prescriber to write directly to adult psychiatry with most up-to-date pharmacological treatment plan and the most up-to-date physical health.
- Child and adolescent mental health services intellectual disability transition coordinator to document via child and adolescent mental health services intellectual disability launch pad discharge or transition or task the care coordinator to add information from single access referral form and transition document.
- Referral accepted: joint transition to commence between care coordinators allocated from child and adolescent mental health services intellectual disability and adult learning disability introduction, meetings, clinic appointments adult learning disability coordinator to be invited.
- Pharmacological treatment for depression or anxiety, adult learning disability psychiatrist to decide prior to the young person turning 18 to accept or signpost to GP for ongoing treatment (melatonin to be accepted). Prescribing to be continued by child and adolescent mental health services intellectual disability until the first appointment with adult learning disability psychiatry.
- If identified no role for adult learning disability, adult learning disability service leaflet to be sent alongside discharge from child and adolescent mental health services intellectual disability to make young persons and carers aware of adult service support if required in the future.
11.7 Appendix G North Lincolnshire child and adolescent mental health services intellectual disability and adult learning disability transition process
- Transition’s cases from child and adolescent mental health services intellectual disabilities to adult learning disabilities to begin from 17 and a half years of age. Cases between 17 and 17 and a half if complex to begin early.
- Child and adolescent mental health services intellectual disability transition agenda to adult learning disability services document to be completed by child and adolescent mental health services intellectual disability transition coordinator.
- Microsoft Teams transition meeting every three months first Monday 9:30am to 10:30am.
- No transition cases or potential transitions to discuss to email rdash.actldnl@nhs.net to cancel the meeting.
- Transition document to outline the following information:
- name
- date of birth
- NHS number
- care coordinator
- other services or professionals involved
- risk: low, medium or high
- proposed pathway
- diagnosis
- identified needs or challenges
- pharmacological treatment plans
- Action points to be documented in section 4 action log via transition document by child and adolescent mental health services intellectual disability transition coordinator.
- Transition document with action points to be disseminated with adult learning disability colleagues and child and adolescent mental health services coordinator of cases.
- Cases that require prescribing input for attention deficit hyperactivity disorder (ADHD) treatment, North Lincolnshire adult neurodevelopmental service form to be completed and emailed to rdash.nl-adhd-al@nhs.net.
- Single access referral form (SARF) to be completed if agreed to do so at transition meeting.
- Psychometric questionnaires to be completed and sent with single access referral form:
- mGASS (if cases prescribed anti-psychotics only)
- easy read Glasgow
- depression and anxiety scale (treating depression or anxiety if patient can participate)
- Formulations, assessment reports, plans and psychiatry clinic letters to be sent with single access referral form. Up-to-date face risk, care plans, at the last transition step to be available via system one for adult learning disability colleagues proposed pathway if for adult psychiatry only, respective child and adolescent mental health services intellectual disability prescriber to write directly to adult psychiatry with most up-to-date pharmacological treatment plan, reason for prescribing and the most up-to-date physical health monitoring information
- Child and adolescent mental health services intellectual disability transition coordinator to document via child and adolescent mental health services intellectual disability launch pad discharge or transition or task the care coordinator to add information from single access referral form and transition document.
- Referral accepted: joint transition to commence between care coordinators allocated from child and adolescent mental health services intellectual disability and adult learning disability introduction, meetings, clinic appointments adult learning disability coordinator to be invited.
- If identified no role for adult learning disability, adult learning disability service leaflet to be sent alongside discharge from child and adolescent mental health services intellectual disabilities to make young persons and carers aware of adult service support if required in the future.
- Pharmacological treatment for depression or anxiety, adult learning disability psychiatrist to decide prior to the young person turning 18 to accept or signpost to GP for ongoing treatment (Melatonin to be accepted). Prescribing to be continued by child and adolescent mental health services intellectual disabilities until the first appointment with adult learning disability psychiatry.
11.8 Appendix H early interventions in psychosis and child and adolescent mental health problems care pathway
11.8.1 Process for under 16-year-olds
- Referral received through:
- already known to child and adolescent mental health services
- referral received by child and adolescent mental health services with suggestion of symptoms of psychosis, initial child and adolescent mental health services assessment
- referral received by early interventions in psychosis for person less than 16 years of age
- Joint assessment completed between child and adolescent mental health services and early interventions in psychosis led by early interventions in psychosis:
- symptoms of psychosis evident (first episode psychosis)
- meets at risk mental state for psychosis (ARMSp) threshold (where at risk mental state (ARMS) pathway is delivered)
- no signs of psychosis but other mental health issues identified
- Outcome of assessment provided to individual or family by Early Intervention team (if first episode psychosis or at risk mental state):
- joint work between child and adolescent mental health services and early interventions in psychosis: lead clinician to be determined by need, joint care plan (medical input, including prescribing) from child and adolescent mental health services consultant psychiatrist) and risk assessment to be developed in collaboration between the services with the individual and family
- taken onto at risk mental state pathway: also child and adolescent mental health services for other identified mental health needs
- taken onto at risk mental state pathway: no input from child and adolescent mental health services identified
- child and adolescent mental health services
11.8.2 Early interventions in psychosis and child and adolescent mental health problems care pathway process for 16 to 18-year-olds
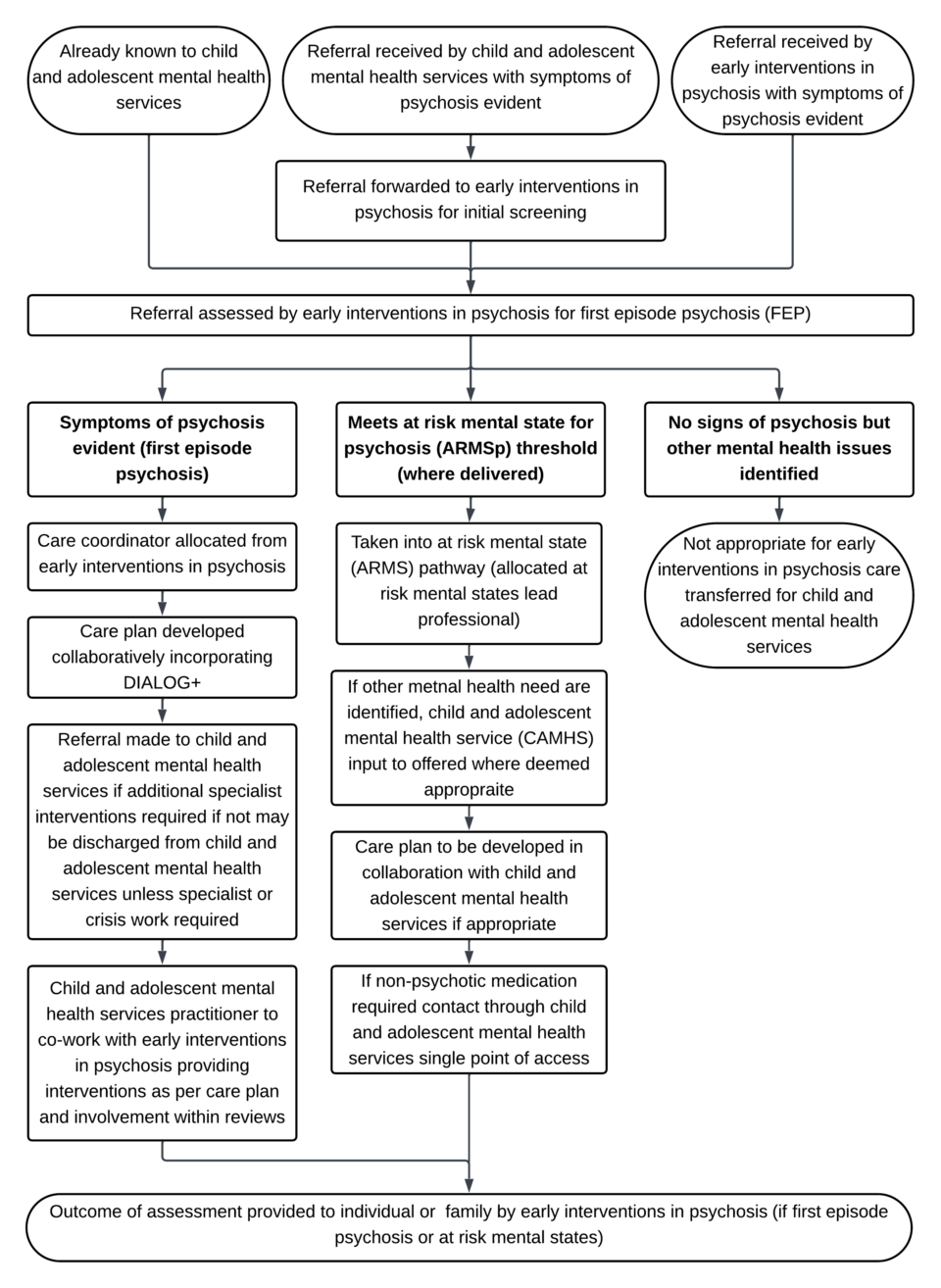
- Referral received through:
- already known to child and adolescent mental health services
- referral received by child and adolescent mental health services with symptoms of psychosis evident, referral forwarded to early interventions in psychosis for initial screening
- referral received by early interventions in psychosis with symptoms of psychosis evident
- Referral assessed by early interventions in psychosis for first episode psychosis (FEP):
- symptoms of psychosis evident (first episode psychosis):
- care coordinator allocated from early interventions in psychosis
- care plan developed collaboratively incorporating DIALOG+
- referral made to child and adolescent mental health services if additional specialist interventions required if not may be discharged from child and adolescent mental health services unless specialist or crisis work required
- child and adolescent mental health services practitioner to co-work with early interventions in psychosis providing interventions as per care plan and involvement within reviews
- meets at risk mental state for psychosis (ARMSp) threshold (where delivered):
- taken into at risk mental state (ARMS) pathway (allocated at risk mental states lead professional)
- if other mental health need are identified, child and adolescent mental health service (CAMHS) input to offered where deemed appropriate
- care plan to be developed in collaboration with child and adolescent mental health services if appropriate
- if non-psychotic medication required contact through child and adolescent mental health services single point of access
- no signs of psychosis but other mental health issues identified: not appropriate for early interventions in psychosis care transferred for child and adolescent mental health services
- symptoms of psychosis evident (first episode psychosis):
- Outcome of assessment provided to individual or family by early interventions in psychosis (if first episode psychosis or at-risk mental states).
11.9 Appendix I transition and joint working between child and adolescent mental health services and talking therapies
11.9.1 Talking therapies inclusion and exclusion criteria for 16 to 18-year-olds
11.9.1.1 Inclusion criteria
- Low risk: only those young people that can be managed by a therapist and GP alone (patients with severe or frequent self-harm should be seen within child and adolescent mental health services).
- Presenting problem is mild to moderate anxiety and depression and patient is requiring treatment for one of the following conditions:
- depression
- generalised anxiety disorder
- panic
- social anxiety
- phobia
- post-traumatic stress disorder (PTSD)
- agoraphobia
- health anxiety
- body dysmorphia disorder
- obsessive compulsive disorder (OCD)
- Young person choosing to be seen in an adult based service whose needs cannot ordinarily be met by child and adolescent mental health services.
- Patient needs to be able to complete routine outcome measures every session including minimum data set of PHQ9, GAD7, WASA or phobia scales and when appropriate an anxiety disorder specific measure (ADSM).
- Patients with long term conditions.
- Patients with severe mental illness (SMI) diagnosis will not be automatically excluded, for example, if stable and able to benefit from standalone intervention not linked to their severe mental illness.
11.9.1.2 Exclusion criteria
- Medium to high risk: those with severe self-harm or present as a significant risk to themselves should be seen within child and adolescent mental health services or by child and adolescent mental health services crisis services.
- Young people at significant risk to other people, for example:
- risk of neglect of children or vulnerable adults
- expressions of high levels of violence or aggression would not be suitable for talking therapies
- Young people who frequently self-harm, depending on the severity of self-harm. Child and adolescent mental health services to assess, but those whose primary problem is related to self-harm should sit within child and adolescent mental health services.
- Those with complexity that means they will require longer than the brief therapy model of a maximum of up to 20 sessions offered within talking therapies.
- Those who require systemic support.
- Those who require specific treatment intervention for diagnosed personality disorder. In certain cases, young people with personality disorder with an additional diagnosis of depression or anxiety, may be offered targeted interventions for these latter conditions, where there is evidence that personality factors would not interfere with effective treatment of these conditions:
- young people who require support for eating disorders
- young people who only require support for self-esteem
- young people whose primary problem is related to drugs or alcohol use, please also see the talking therapies drug and alcohol policy
- those whose primary problem is addiction related
- anyone with forensic history that may present as a risk to others
- those with severe learning disabilities
- anyone with cognitive impairment
- patients with attention deficit hyperactivity disorder (ADHD) who require medication (patients with neurodiversity to be considered on case-by-case basis and in order to benefit from talking therapies, neurodiversity needs not to be better met by child and adolescent mental health services)
11.9.2 Talking therapies process
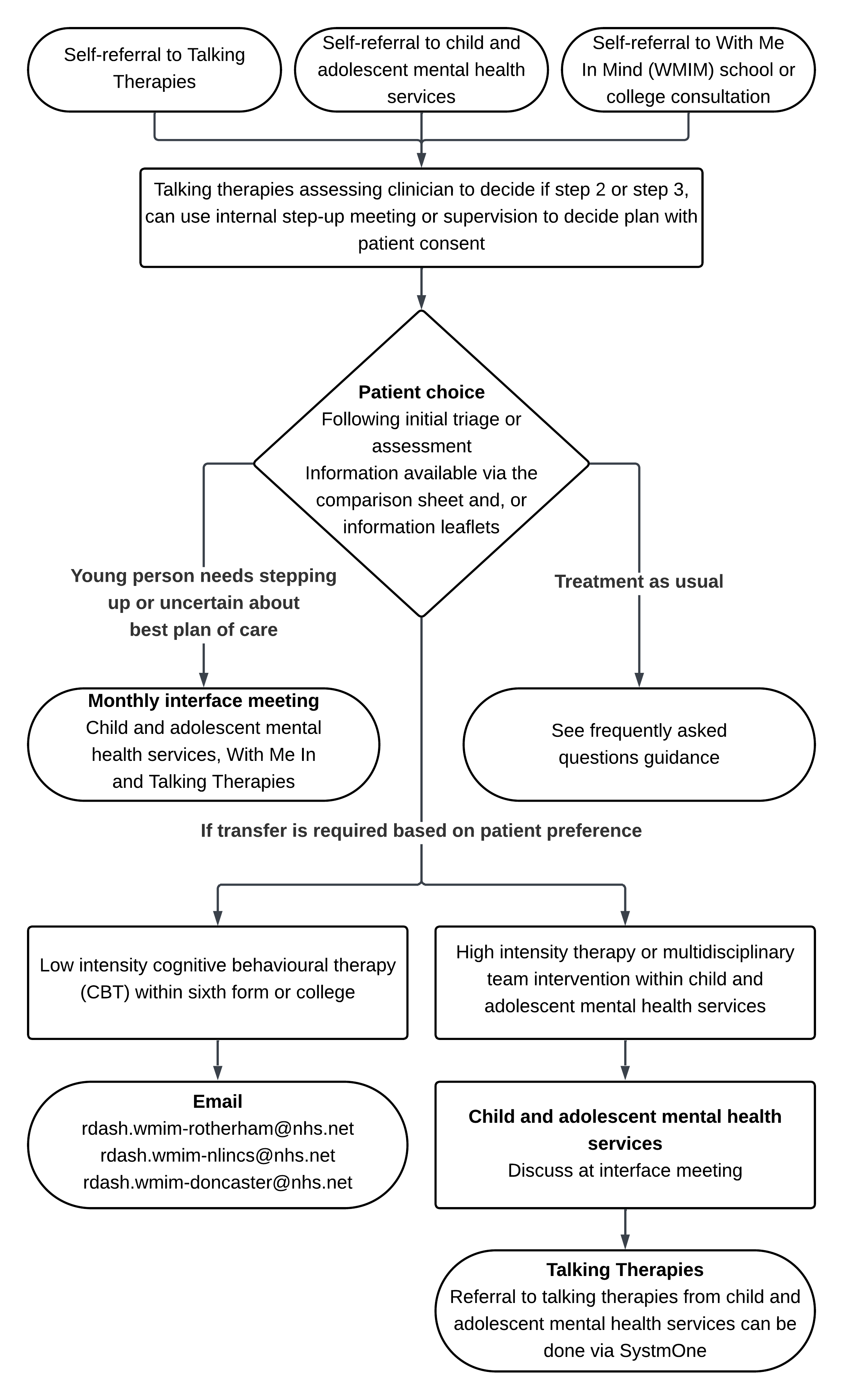
- Self-referral received through:
- Talking Therapies
- Child and adolescent mental health services
- With Me In Mind (WMIM) school or college consultation
- Talking therapies: assessing clinician to decide if step 2 or step 3, can use internal step-up meeting or supervision to decide plan with patient consent.
- Patient choice: following initial triage or assessment
Information available via the comparison sheet and, or information leaflets. - Transfer is required based on patient preference:
- low intensity cognitive behavioural therapy (CBT)
within sixth form or college then email With Me in Mind: - high intensity therapy or multidisciplinary team intervention within child and adolescent mental health services:
- discuss at interface meeting talking therapies
- referral to talking therapies from child and adolescent mental health services can be done via SystmOne
- low intensity cognitive behavioural therapy (CBT)
- Young person needs stepping up or uncertain about best plan of care: monthly interface meeting attendees:
- Child and adolescent mental health services
- With Me In Mind
- Talking Therapies
- Treatment as usual: see frequently asked questions guidance.
11.9.3 Treatment as usual within talking therapies
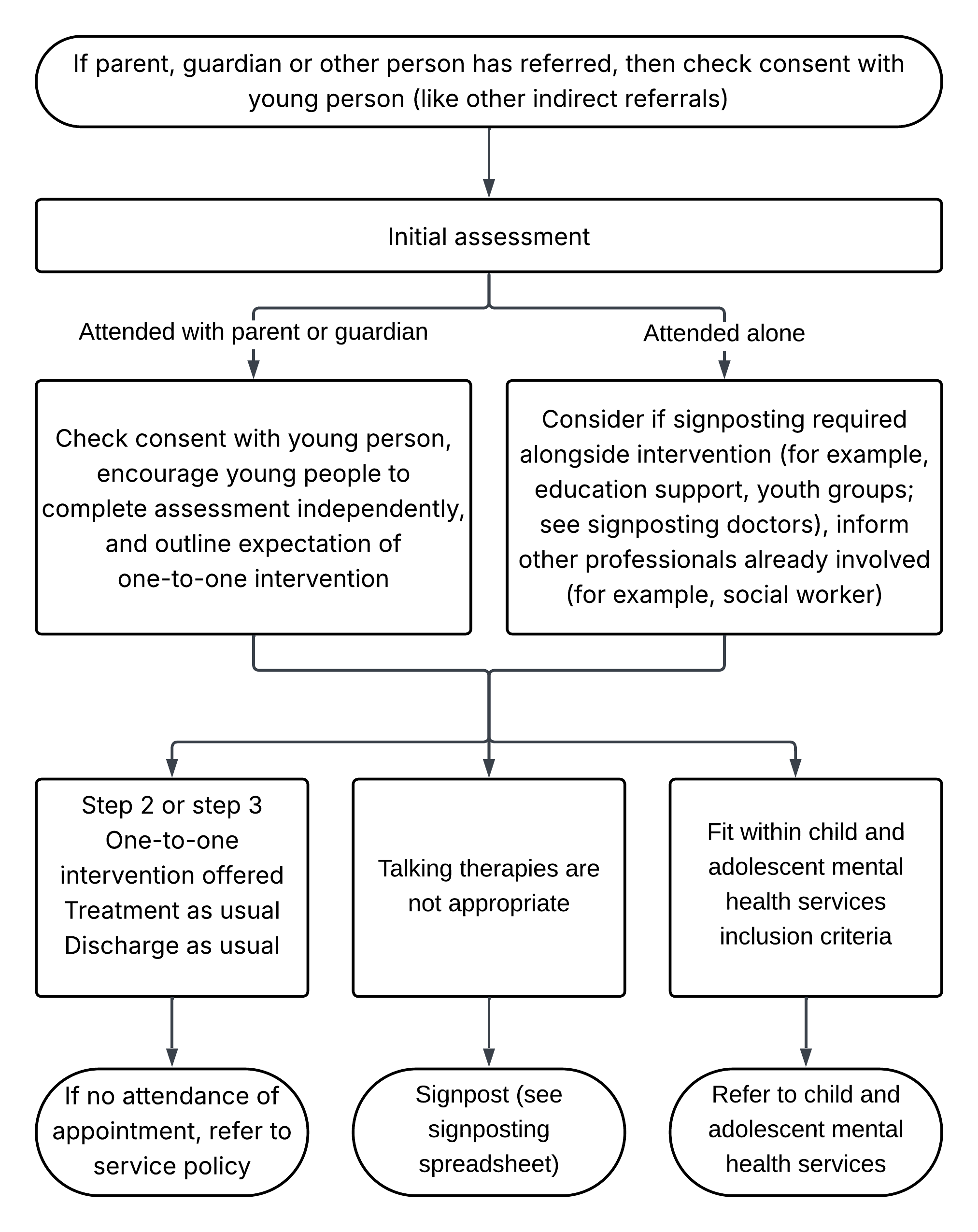
- If parent, guardian or other person has referred, then check consent with young person (like other indirect referrals).
- Initial assessment:
- attended with parent or guardian: check consent with young person, encourage young people to complete assessment independently, and outline expectation of one-to-one intervention
- attended alone: consider if signposting required alongside intervention (for example, education support, youth groups; see signposting doctors), inform other professionals already involved (for example, social worker)
- After assessment:
- talking therapies:
- step 2 or step 3
- one-to-one intervention offered
- treatment as usual
- discharge as usual
- if no attendance of appointment, refer to service policy
- talking therapies are not appropriate: signpost (see signposting spreadsheet)
- fit within child and adolescent mental health services inclusion criteria: refer to child and adolescent mental health services
- talking therapies:
Document control
- Version: 7.1.
- Unique reference number: 49.
- Approved by: clinical effectiveness meeting
- Date approved: 9 September 2025.
- Name of originator or author: director of nursing.
- Name of responsible individual: chief nursing officer.
- Date issued: 24 March 2026.
- Review date: 31 March 2029.
- Target audience: clinical staff, particularly children and young people’s mental health services (CAMHS), adult mental health services and learning disability services.
Page last reviewed: April 20, 2026
Next review due: April 20, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.