1 Policy summary
This policy details the trust approach and expected standards in the use of a vision based patient monitoring system (VBPMS). This assistive tool enables colleagues to enhance and support patient safety in inpatient services by delivering noncontact measurement of physiological parameters such as pulse and breathing rate, some degree of patient location, activity or behaviour data and some form of contextual video information (which may be blurred) either in real time or through subsequent reviews. The use of this system is intended to compliment clinical practice and not replace the need for good nursing interventions.
Vision based patient monitoring systems must be prescribed in a person-centred way and supported by clear and frequent communication, regular reviews by the multidisciplinary team (MDT), clear and collaborative care planning, and therapeutic engagement with the clinical team.
Data captured by the vision based patient monitoring system is used by Rotherham, Doncaster and South Humber Trust (RDaSH) to enhance patient safety and activity monitoring regimes.
2 Introduction
The trust is utilising vision based patient monitoring system to enhance the delivery of safe and effective mental health care by introducing solutions to proactively manage and prevent incidents.
The trust has considered the national recommendations, guidance and best practice on safe use of vision based patient monitoring systems in the development of this policy.
This policy details the processes to be followed when using vision based patient monitoring systems. The use of the system will align to and compliment traditional working practices and relevant trust policies.
Vision based patient monitoring does not replace positive and therapeutic engagement with patients and the visible presence of colleagues within inpatient settings. Colleagues must remain responsible for the patient and clinical judgement must always be used.
3 Purpose
The purpose of this document is to provide colleagues with clear guidance on vision based patient monitoring systems, to help plan, review and optimise treatment for patients whilst making the best use of resources.
The trust currently deliver vision based patient monitoring system via LIO which uses an optical sensor (camera and infrared illumination in a secure housing on the wall and is operational 24 hours a day, 7 days a week) supporting colleagues to:
- take cardio-respiratory measurements remotely
- access cardio-respiratory trends from the last 24 hours to understand if a resting patient’s physical health may be deteriorating
- receive real time alerts to high-risk activity, prompting a safety check
- view objective patient activity reports to support clinical decision-making
The technology is not closed-circuit television (CCTV), and colleagues should not attempt to use it in this way. Colleagues should refer to the trust security policy for further information on CCTV.
4 Scope
This document is intended for use by colleagues where LIO is deployed. Please refer to the LIO (staff access only) on the intranet for further details of where and how LIO is deployed across the trust.
The policy should be read in conjunction with:
- supportive therapeutic observation policy
- physical health policy
- patient falls manual (prevention and management)
- resuscitation manual
- consent to care and treatment policy
- healthcare record keeping policy
- Mental Capacity Act policy
For further information about responsibilities, accountabilities and duties of all colleagues, please refer to appendix A.
5 Procedure
LIO is available for use in patient and seclusion rooms across all adult and older adult mental health inpatient services to enhance and support patient safety.
5.1 Quick guide
5.1.1 Competency and training
Training for LIO is delivered through an online platform called OxeAcademy.
Prior to using the system, colleagues not previously trained must complete the online training package and obtain a digital certificate.
This should be given to their line manager who will ensure it is uploaded to electronic staff record (ESR) via the Learning and Development team.
5.1.2 Patient Information
Colleagues must ensure that patients and family, carers and visitors are informed on admission that the trust utilise LIO to promote safety.
An information pack should be provided to patients on admission detailing what, when and how patient activity and pulse and respiration rates are monitored.
5.1.3 Consent and capacity
Patients should be able to discuss queries or concerns they may have about LIO with the clinical team including objecting to it use.
If capacity is doubted a MCA1 form should be undertaken. If a patient is accessed as lacking capacity a best interest’s decision should be made including family or carer’s view and evidenced on MCA2 form.
5.1.4 Physical observation
LIO can be used to monitor pulse and respiration rates only.
Where a patient requires regular physical observations, it is expected that the pulse and respiration are taken manually alongside other identified physical observations, not a combination of LIO and manual.
5.1.5 Therapeutic observations
Where deemed clinically appropriate, LIO enables the patient to be monitored without having to physically enter their room to undertake the observation. This could promote sleep at night or reduce agitation.
5.1.6 Seclusion
LIO must never be paused in the seclusion environment.
5.1.7 Incidents
Any request for video footage must be directly linked to a patient related incident.
Request for data can be made by all registered professionals of the multidisciplinary team to support@liohealth.com or by contacting customer services on 0800 030 6781. Full guidance can be read in 6.10.
5.2 General guidance and principles of use
- All patients and their family, carers and visitors must be informed on admission that the trust utilise LIO to promote safety.
- Any decision to use LIO should be made on a case-by-case basis in a person-centred way.
- The use of LIO should be on the basis that there is a legitimate and proportionate aim that is both lawful and fair and it should not be assumed by colleagues that it is to be implemented for each patient in a blanket way.
- Where a decision has been made to use or not use LIO, the discussion with the patient and other relevant people where appropriate, such as carer or family, other members of the multidisciplinary team, as well as the intended aims of use should be recorded in the electronic patient record (EPR).
- All patients must have an LIO care plan in place reflecting their decision. Colleagues must use and personalise the standard LIO care plan in SystmOne.
- It is the responsibility of the nurse in charge to ensure that LIO is used only by colleagues who are suitably trained. Please refer to section 6 training implications for further guidance.
- When undertaking an observation, it is important that a patient’s privacy and dignity is adequately considered and protected. There may be instances when it is not appropriate to continue with an observation, for example:
- if a patient is in a state of undress
- patient is engaging in sexual activity (masturbation)
- if a patient is privately observing religious beliefs
- An observation should be cancelled immediately in these circumstances if no risk is evident and reattempted later.
- When an alert is received or a check is performed, colleagues will see a live stream of the patient for 15 seconds only, alerts are blurred images.
- All incidents observed or highlighted via LIO must be reported in line with the trust incident management policy and recorded in the electronic patient record in line with appendix E recording LIO incidents in SystmOne.
- The system does not provide alerts for vital signs, for example alerts for high or low pulse and, or breathing rate or cessation of vital signs.
5.3 System functionality
LIO has 3 core functions that can be used independently or collectively to support therapeutic and physical health observations:
- observations
- vital signs
- alerts
On admission and where appropriate thereafter, colleagues and subsequently the multidisciplinary team should consider the clinical benefits of each function, and if they should be offered and, or used to support the patient.
Colleagues should refer and adhere to the respective polices relating to observations to ensure appropriate clinical considerations and decision-making is undertaken.
The electronic patient record must reflect the decisions to use the varying functionality, including the clinical rational. Where a decision to use LIO as an alternative to manual or in person observations in reached, this must be clearly rationalised, documented and should be reflected in the patient care plan.
A useful flowchart on assisted observations can be found in appendix C.
Any requests for changes to functionality should be sent to rdash.cso@nhs.net for consideration and approval.
LIO should not be used if a patient is using the ensuite bathroom, the room tile will clearly indicate the room status. Colleagues must only open the vital signs workflow when the room tile is green and the room tile is “in room” or “in bed”.
5.3.1 Observations
LIO may be a helpful addition to support in person observations:
- if entering the patient’s bedroom causes them to become more agitated and distressed
- informing whether another patient has entered the room through a room entry alert
LIO allows for the patient to be monitored without having to physically enter their room to undertake the observation. Colleagues can only rely on the use of the LIO to support these observations, with visual assurance that the patient is either awake and alert, or asleep with clear signs of breathing via the video functionality, in addition to taking a pulse and respiration reading. This functionality should not be routinely used during the day when colleagues should continue to undertake in person visual checks. If there are any concerns regarding the patient’s presentation or any uncertainty regarding the patient’s health via the camera or pulse and respiration reading, colleagues must complete an in-person assessment.
5.3.2 Physical health observations (vital signs)
LIO records the basic health observations of pulse and respiration. If additional physical health readings are required, such as blood pressure and oxygen saturation levels, this should be completed in line with relevant trust process. When physical health observations are taken, colleagues will see a live stream of the patient for 15 seconds only.
Where a patient requires regular physical observations, it is expected that the pulse and respiration rates are taken manually alongside other identified physical observations, not a combination of LIO and manual.
LIO does not measure pulse and respiration rate when a patient is moving. Upon observation, if the patient is moving, record their position and reattempt when the patient is still.
Colleagues can make two attempts to establish a patient’s breathing rate via LIO before physically locating the patient and manually measuring their breathing rate.
If colleagues have any concerns about the patient’s physical state, they must escalate as per the trust’s physical health policy. If a reading (pulse or respiration rate) is abnormal, colleagues should confirm the reading manually before escalating unless there are clear visual signs of deterioration.
LIO vital signs is a certified medical device, however, if there are any concerns when using the system, patients should be assessed in person.
Emergency intervention does not need to be delayed by first checking LIO. Clinical judgement should be exercised to determine the most appropriate response for each situation.
5.3.3 Alerts
LIO provides information and notifications to colleagues about a patient’s location in their room.
When an alert is sounded, colleagues can initially view the alert through an anonymised (blurred) image and assess if a physical check is necessary to maintain patient safety.
Colleagues have the option to temporarily pause these alerts for up to 30 minutes while they are delivering personal care to individual patients.
The replay last alert function enables colleagues to view an anonymised (blurred) clip of the last alert that was triggered in a patient room. The clip will show 5 minutes before and after the alert, allowing colleagues to review why the alert was triggered and help determine the appropriate course of action they should take. Only the last alert triggered is viewable within a 24-hour period.
Colleagues should also consider the need to preserve data longer term for further investigation and should refer to section 6.10 requesting and approving data for investigation for further guidance.
5.4 Seclusion
LIO is intended to enhance the visual and physical observation detailed in the seclusion policy, it cannot replace the need for constant observation but offers additional intelligence and may enable colleagues to monitor the patient’s physical health more frequently and without having to enter the seclusion room where such action may increase risk or distress.
LIO should not be paused in the seclusion environment as it is an additional aid to support a patient who is already subject to constant observation.
A mobile LIO tablet will be located within seclusion areas and should be activated on admittance of a patient, enabling colleagues to monitor the patient in line with this policy.
5.5 Falls
LIO can be used to assist with falls prevention and management by:
- alerting colleagues when the patient is in the process of exiting the bed through a leaving bed alert
- alerting colleagues when the patient is out of their bed through an out of bed alert
- notifying colleagues when the patient enters the bathroom
- viewing footage after a patient has fallen to check for any contributing factors, so subsequent mitigations can be applied
5.6 Changes to room layout
LIO can automatically detect when a bed is moved slightly, for example, for cleaning, and when a bed is raised and lowered.
However, LIO cannot automatically detect when a bed is moved significantly, for example: to the other side of the room or rotated by 90 degrees. This could affect the accuracy of “in bed” room states and some alerts, particularly leaving bed and out of bed alerts.
If a bed has been moved significantly from its original position, colleagues must inform LIO as soon as possible via the Feedback button within the app or via the 24 hours a day, 7 days a week support line (0800 030 6781) so appropriate adjustments can be made. LIO must also be informed if the furniture within a room has moved, for example, wardrobes or other large items, so they can ensure the optical sensor is not obscured.
5.7 Patient information
On admission, and where appropriate thereafter, colleagues will discuss the purpose of LIO with the patient, including, how it works in relation to patient activity, pulse and respiration rates and issues of privacy, which may be compromised when an observation is attempted. This discussion will be supported by written information and must include a patient leaflet (staff access only).
There are also options available to the patient regarding how LIO can be implemented, including the alert system alone being utilised (for example, colleagues not accessing the camera or vital signs functionality unless triggered by an alert).
Patients should be encouraged to explore any queries or concerns they have, and colleagues should address these where possible or escalate where support is required. Colleagues should utilise the wider resource available on LIO (staff access only) on the intranet to support these conversations.
The outcome of this discussion should capture the patient’s choice regarding the use of LIO and must be recorded in the electronic patient record.
If LIO is to be used, further exploration regarding privacy should determine what the patient would like to happen if a compromise occurs. This may include informing the patient regarding what was observed, or simply a polite reminder that LIO is in operation. The steps agreed must be detailed in the care plan.
LIO signage showing the use of the equipment must be displayed clearly in public areas. Colleagues should refer to LIO (staff access only) on the intranet to access and print the patient poster.
Information around LIO should be shared with the patient’s family, carers, and visitors at the earliest opportunity.
More information about how the trust uses data is outlined in the trust’s privacy notice or by contacting the data protection officer (DPO) or the Information Governance team.
5.8 Making a decision regarding the use of LIO
On admission the admitting nurse will consult with the multidisciplinary team and consider the clinical appropriateness of LIO, taking into account the best interest of the patient, balancing individual preference, safety, risk management and alternative options, just as they would other treatment approaches. Support should be requested from senior colleagues where appropriate, including on call support structures out of hours.
Where LIO is deemed clinically appropriate to support care, and the patient objects at any point during admission, consideration should first be given to their capacity to make a decision about the use of LIO. If there are no concerns regarding capacity, the decision should be respected if clinically appropriate.
If capacity to consent regarding LIO is doubted, an assessment of capacity must be undertaken. If the patient lacks capacity to make the decision, a decision must be made by the multidisciplinary team in the patient’s best interests. Colleagues should refer to the trust’s Mental Capacity Act policy for further guidance. This process should be followed for both informal and detained patients.
All decisions relating to the use or withdrawal of LIO, including best interest decisions, must be reviewed by the responsible clinician (RC), consultant in charge, approved clinician (AC), consultant on call and the multidisciplinary team as soon as is practicable within 24 hours. As these decisions are not medical emergencies, the multidisciplinary team discussions should ordinarily take place during the day shift hours.
This approach needs open and honest communication with the patient and their representatives. Patients should be supported where appropriate to approach advocacy services as follows:
All decisions relating to the use or withdrawal of LIO must be reflected in the care plan to ensure the multidisciplinary team retain oversight and tailor treatment accordingly. Decisions should be reviewed weekly, in line with relevant legislation or where there is a significant change in presentation.
A quick glance decision-making flow chart can be found in appendix D.
Please note, if the system is switched off for an individual room, it must be manually switched back on again when required. A LIO check should be performed for each admission to ensure the system is active and working correctly.
5.9 Functionality development approval process
To submit a change request regarding functionality, colleagues must follow the steps below.
- Complete LIO feedback form via the LIO system, LIO to acknowledge receipt and seek clarity where required.
- LIO to seek approval from trust Patient Safety Leadership team or directors of nursing or matron and service manager.
- LIO to consider viability of request and advise on challenges or blockers.
- LIO to action change and confirm with trust.
5.10 Requesting and approving data for investigation
LIO data (video footage and analytics) can be used to support investigations. Video footage must be requested and provided by LIO as described in the process below. Any request for video footage should be directly linked to a patient safety incident. However, there may be instances where other concerns are observed when viewing video footage that may require further investigation.
Video footage is available in clear and anonymised (blurred) formats depending on how quickly data is requested. Clear video footage is only available for 24 hours from the point of recording.
- Requests for data can be made by all registered professionals of the multidisciplinary team to support@liohealth.com or by contacting customer services on 0800 030 6781. The incident report (IR1) number must be referenced in the request to support the authoriser in the decision to release footage.
- The patient should be informed when footage has been requested via Egress and colleagues should record in the electronic patient record when footage has been obtained.
- LIO will save the data and request permission via an electronic release form to the trust from the Patient Safety Leadership team (PSLT) or directors of nursing or matron and service manager.
- The Patient Safety Leadership team or directors of nursing or matron and service manager will consider where appropriate to approve the request.
- Once approved, LIO will load the video into the Egress secure portal. This will send a secure email to the designated care group or Patient Safety Leadership team mailbox with a link to download the video which can be downloaded within 29 days from the Egress portal.
- The designated mailbox recipients will contact the server and storage specialist in information technology (IT) services or the IT service desk to log a call, inform of a new incident and request that a new top-level digital folder is created in the trust’s secure video folder (R:\secure video).
- The IR1 number for the respective incident will determine the folder name (for example, IR1.134508).
- The designated mailbox recipients will:
- have permission to store and save footage into the sub folders
- create a sub folder for each incident which should be named in reference to the incident date and location for example, 20210810_Woodlands
- determine appropriate access and add permissions accordingly
- upload the video footage and ensure it can be viewed in full from the new location
- to enable trust devices to view the video footage colleagues may need to change their default app for “.avi” type to photos, click on the search icon in the bottom right, type default, select default apps, select choose default application by file type, find “.avi” and select photos or the media player you want to use. Colleagues can contact IT if further assistance is required
- retain the video footage until any associated investigation is concluded
- Outside of normal working hours, where there is a clinical need to view footage urgently, the nurse in charge should seek approval from the on-call manager. Footage should be viewed directly from the Egress portal and standard process should resume for saving, retention and deletion.
Where there are data protection queries or a request to use video footage outside its original purpose, colleagues should liaise with the data protection officer (DPO) for advice and guidance.
The lead investigator should consider how colleagues will be supported and debriefed when viewing footage.
See appendix F for LIO process guide in full.
5.11 Data retention and deletion
Footage stored on the trust’s secure video folder (R:\Secure Video) must be retained in line with NHS record code of practice. Retention timescales may vary depending on the original reason for storage.
5.12 Oversight
The partnership board meets quarterly and provides the trust and LIO with the opportunity to discuss overall use of the system, developments and highlight any issues that need to be resolved.
The digital community of practice meets bimonthly and provides an opportunity for clinicians and front-end users of the system to reflect on practice, raise issues for discussion and action directly with LIO, it also provides an opportunity for LIO to share developments directly with trust colleagues.
5.13 Business continuity plan
If for any reason there is a technical failure or malfunction of LIO, then colleagues must revert to the manual taking and recording of observations and ensure that the appropriate supporting clinical policies and any local working instructions or agreements are followed.
All faults should be reported to LIO. Any connection issues need to be reported to both LIO and trust IT service desk.
Please also refer to your local business continuity plan.
5.14 Escalations
Concerns regarding LIO functionality should be escalated to the ward manager and LIO.
Concerns regarding consent, privacy and information governance should be escalated to the mental capacity lead and head of information governance respectively.
Concerns regarding safety should be raised with line managers and the Patient Safety Leadership team or via freedom to speak up (staff access only).
6 Training implications
Training for LIO is delivered through an online learning platform called OxeAcademy offering refresher training and user guides. Colleagues can sign up with their trust email, and by selecting “RDaSH” from the “organisation name” drop down.
Prior to using the system, colleagues not previously trained must complete the online training package and obtain a digital certificate. Colleagues should provide a copy of this certificate to their line manager who will ensure it is uploaded to electronic staff record (ESR) via the trust’s Learning and Development team at rdash.learninganddevtraining@nhs.net.
LIO will provide the learning and development team with a monthly report. Learning and development will monitor trust compliance within electronic staff record, escalate any immediate concerns to the respective care group and provide monthly oversight reports.
Each ward will have LIO champions who are responsible for supporting colleagues with the system.
It is the responsibility of each matron to ensure they have sufficient LIO champions to support the use of LIO in practice.
It is important that colleagues using the system provide regular feedback (sent via the monitor) to support troubleshooting.
Additional technical support will be provided by LIO via:
- support@liohealth.com
- 0800 030 6781 (customer service phone line for urgent technical issues)
Most technical issues will be resolved remotely. Where onsite support is required from LIO, attendance will be between 24 and 72 hours provided access can be facilitated.
7 Equality impact assessment screening
To access the equality impact assessment for this policy, please email rdash.equalityanddiversity@nhs.net to request the document.
7.1 Privacy, dignity and respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, ‘not just clinically but in terms of dignity and respect’.
As a consequence the trust is required to articulate its intent to deliver care with privacy and dignity that treats all service users with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
7.1.1 How this will be met
All colleagues, contractors and partner organisations working on behalf of the trust must follow the requirements of this policy and other related policies, particularly those relating to information governance. All health professionals must also meet their own professional codes of conduct in relation to confidentiality.
7.2 Mental Capacity Act (2005)
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals’ capacity to participate in the decision-making process. Consequently, no intervention should be carried out without either the individual’s informed consent, or the powers included in a legal framework, or by order of the court.
Therefore, the trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act (2005). For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act (2005) to ensure for that the rights of individual are protected and they are supported to make their own decisions where possible and that any decisions made on their behalf when they lack capacity are made in their best interests and least restrictive of their rights and freedoms.
7.2.1 How this will be met
All individuals involved in the implementation of this policy should do so in accordance with the guiding principles of the mental capacity Act 2005.
8 Links to any other associated documents
- LIO
- Trust incident management policy
- Trust’s privacy notice
- Information Governance team
- Mental Capacity Act policy
- Resuscitation manual
- security policy
- Supportive therapeutic observation policy
- Patient falls manual (prevention and management)
- Physical health policy
- NHS record code of practice
- Freedom to speak up (staff access only)
- Consent to care and treatment policy
- Healthcare record keeping policy
9 References
10 Appendices
10.1 Appendix A responsibilities, accountabilities and duties
10.1.1 The trust
The trust has a duty of care to ensure that all aspects of patient safety are properly managed and where appropriate the trust has the correct assistive tools in place to enhance and support patient safety. The trust must adhere to the legislative, statutory, and good practice guidance.
10.1.2 Chief executive
The chief executive has overall accountability and responsibility for patient safety within the trust. This function is delegated to the executive medical director and the executive director of nursing and allied health professionals, who are responsible for driving high quality safety standards ensuring that the correct infrastructures and systems are in place.
10.1.3 Medical director and the executive director of nursing and allied health professionals
The trust’s executive medical director and the executive director of nursing and allied health professionals are responsible for driving high quality safety standards ensuring that the correct infrastructures and systems are in place.
10.1.4 Caldicott guardian
Caldicott guardian is responsible for protecting the confidentiality of patient and service user information and enabling appropriate information sharing.
10.1.5 Senior information risk owner (SIRO)
Senior information risk owner (SIRO) is an executive board member with allocated lead responsibility for the organisation’s information risks.
10.1.6 Data protection officer
Data protection officer is responsible for ensuring the organisation processes, the personal data of its colleagues, customers, providers or any other individuals (also referred to as data subjects) in compliance with the applicable data protection rules.
10.1.7 Chief nursing information officer
The chief nursing information officer and clinical safety officer is responsible for ensuring that assistive tools are clinically appropriate and adhere to clinical safety guidelines.
10.1.8 Patient Safety Leadership team
The Patient Safety Leadership team are responsible for oversight of the LIO contract, developments to the system and authorising release of secure data.
10.1.9 Senior managers
Senior managers of the trust are responsible for ensuring that assistive tools are appropriately deployed and used in their clinical areas.
10.1.10 Ward managers
Ward managers are responsible for ensuring assistive tools are used appropriately within their ward environments including monitoring colleagues training and compliance and requesting developments to the system and secure data for patient safety incidents.
10.1.11 Nurse in charge
The nurse in charge is responsible for ensuring appropriately trained colleagues use the system.
10.1.12 LIO champions
LIO champions are responsible for completing the train the trainer education programme and ensuring identified colleagues are trained competently. LIO champions should also remain engaged with LIO regarding refresher training and product updates.
10.1.13 Ward based colleagues
Ward based colleagues are responsible for using the system in line with this policy and training.
10.1.4 The multidisciplinary team
The multidisciplinary team (MDT) is responsible for the use or non use and review of LIO supported by the responsible clinician.
10.2 Appendix B monitoring arrangement
10.2.1 Incidents
All incidents must be reported using the trust’s safeguard incident reporting system (IR1). When recording an incident involving the LIO system, colleagues should indicate this on the incident form using the appropriate tick box.
Incidents will be subject to review by the matron for the service, and the head of patient safety (patient safety specialist).
10.2.2 Reporting
Ward managers will monitor compliance with policy, care plans and Mental Capacity Act assessments through localised documentation audits and RePortal reports.
Matrons will oversee compliance through the trust RePortal and oversight and escalation of ward audits.
LIO will provide monthly usage reports which will be provided to care groups for oversight including theme and trend analysis.
LIO monthly local audit to be completed by the ward management team via the electronic audit system and results to be provided to care groups for oversight.
10.3 Appendix C assisted observations process flowchart

- Click on “Take Observation”.
- Check video for patient presence:
- not present, proceed to 10.3.1 check patient
- Check video for reasons for patient concern:
- concerned, proceed to 10.3.1 check patient
- Not concerned, is patient still?
- No, record patient location
- Yes patient is still, is breathing rate available?
- Yes, record patient position, and breathing rate.
- No, if breathing rate not observed, process may be repeated once before checking patient in person is required, proceed to step 1 and repeat process.
10.3.1 Check patient
- Check patient in person.
- Record patient location.
10.4 Appendix D quick glance decision-making flowchart

- Fully inform: make use of materials contained within the resource pack. These materials should be made available in all accessible formats for example, different languages, video, easy read, Braille and so on.
- Document discussion in patient record and make an interim decision regarding use of the system.
- Multidisciplinary team (MDT) meeting should reach a clinical decision regarding the use of the vision based patient monitoring system considering the risk of patient harm and, if relevant, the particular risk of re-traumatisation based on patient history. Multidisciplinary team meeting should also consider whether the patient is admitted informally or formally (subject to the Mental Health Act). The risks and rationale for the decision should be documented in the patient record.
- The best interests meeting will involve patients, family, carers or advocates to discuss the clinical recommendation and rationale and to ensure all views have been considered. A final decision confirmed about whether the system is kept on or switched off will be made.
- Decision to keep the vision based patient monitoring system on or off should be documented in the patient record.
- The use of the vision based patient monitoring system should be discussed weekly with the patient, family or carers as part of their multidisciplinary team care review, or where there is a significant change in presentation. If a consenting patient subsequently objects, the provider should discuss this at the multidisciplinary team meeting and follow the process from step 3.
- If the system is switched off, relevant policies and procedures should be followed.
10.5 Appendix E recording LIO incidents in SystmOne
Colleagues must record in SystmOne when LIO notifies them of a potential incident.
- Select the “RDaSH intervention and de-escalation” tab from the “RRI node” on the clinical tree.
- Left-click on the icon on the view to launch the template.
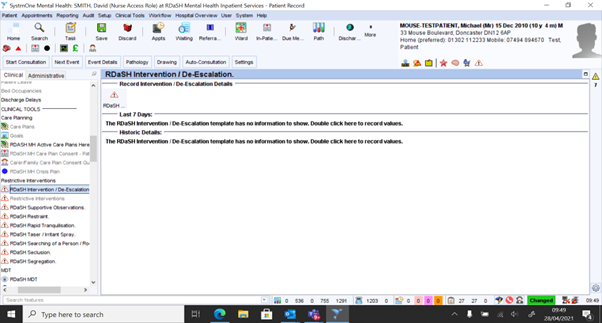
- Complete the date and time field at the top of the template to indicate when LIO made the notification.
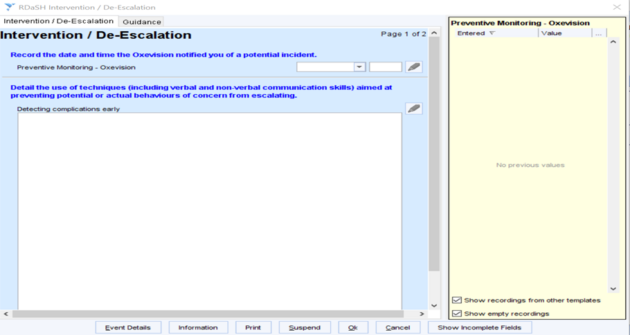
- Complete the remainder of the template as appropriate.
- Save the record.
10.6 Appendix F LIO system, change to clear video data delivery method, process outline
10.6.1 Purpose
This document is to brief LIO customers on the proposed change to how clear video data (CVD) is delivered by LIO to LIO users. It is intended to provide a high-level outline of the workflow, to highlight what the proposed alternative delivery method is and to provide an overview of the workflow for obtaining delivery.
10.6.2 Overview
The LIO system can be used to provide short “videos” of clear video data, typically requested to support an investigation into serious incidents in line with local policies.
LIO deliver the clear video data videos within 72 hours (if requested Monday to Thursday, or 96 hours if requested Friday to Sunday) of the trust authorisation for the video to be delivered. Videos must be requested as soon as possible as the video data is stored on a rolling 24-hour buffer and once the 24-hour limit is reached, the data is permanently lost.
These factors are not being changed as a result of this proposed change.
The proposed change is to deliver the clear video data via an email link to a secure portal (using a secure third-party cloud service called Egress) rather than delivering it by hand, in person, using a secure universal serial bus (USB) stick. The reason for this change is to promote efficient delivery and to increase environmental sustainability.
10.6.3 What is changing
From LIO 1.74 (expected for release in January 2024), customers may receive clear video data videos using the Egress service.
The difference in the overall process is highlighted below:
| Old process | New process |
|---|---|
| Customer requests video | Customer requests video |
| LIO make the video | LIO make the video |
| LIO requests documented authorization to deliver the video | LIO requests documented authorization to deliver the video |
| LIO deliver the video in person via a secure USB stick | LIO deliver the video remotely via secure portal (Egress cloud) |
10.6.4 Overview of the new process
- The health care professional (HCP) will make contact with LIO to request clear video data. This needs to include details of the site, the ward, the room and the time periods (from and to). Requests can be made at any time, 24 hours and 7 days but must be made as soon as possible within 24 hours from the requested start time of the video as video data is automatically deleted after 24 hours.
- LIO will clip the requested clear video data on receipt of the request which secures the video data beyond the 24-hour buffer.
- Once video data is clipped, LIO will seek written authorization from the customer’s designated authorising personnel by emailing a release form to be electronically signed. This release form requests contact information of who is authorised to receive the video. Note, the authorising person has 28 days to approve the release of the video, during which time LIO will follow up at least 4 times. At the end of the 28-day period LIO will close the ticket handling the clear video data release request and the data will be deleted.
- Once the authorising person has electronically signed the release form, LIO will load the video into the Egress secure portal. This will send a secure email to the authorised recipient of the video (as specified on the electronically signed release form) with a link to download the video.
- The recipient of the secure email will then have 29 days to download the video from the Egress portal. LIO will check if the video has been downloaded 10 days after sending the link. If the video has not been downloaded, then LIO will call the recipient to remind them.
- LIO will permanently delete the video and close the request ticket 29 days after the link was sent. No other copies of the data are stored at the customer site or on LIO’s systems.
Note, customers are reminded that once videos are received by them, responsibility for the secure handling of this data is the customer’s responsibility.
10.6.5 About the Egress system
This process takes no more than a couple of minutes (including setting up an Egress account for the first time), although the time to download the video will depend on the requested length of the video and the bandwidth of the recipient’s internet connection. Customers may download the video as many times as they wish during the 29 days after receiving the link by email.
Note, LIO recommend that customer IT departments are notified of the expected use of the Egress system and that IT departments ensure this website or service is allocated onto the organisation’s list of approved and sustained services in line with relevant procedures, for example, ISO 27001.
Specifically, customer’s IT departments will need to “whitelist” the LIO Egress cloud.
LIO recommend using the latest versions of the following browsers to use the Egress service, Google Chrome, Microsoft Edge or Apple Safari. LIO recommends using a desk-based PC to access Egress and not mobile devices. All devices, browsers and systems used to access Egress should be tested by the customer information technology (IT) department before moving to clear video data delivery by Egress.
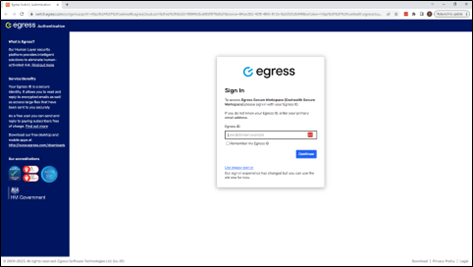
10.6.6 Egress email and download process
The process of receiving the email from Egress and downloading the video is shown below:
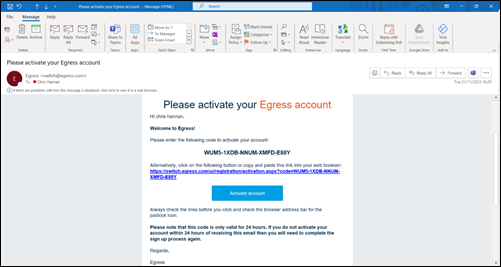
- You will receive an email from workspace@egresscloud.com titled “nameofLIOcolleague shared file_name_AVI_nnn_n_nMG.avi with you”.
An example of the secure email is shown below:

- Click on “view secure content”.

- You will be required to set up an account if you have not done so before. Type in your work email address.
- Complete the account setup questions and click on “create account”.

- A new window will appear requiring an activation code.
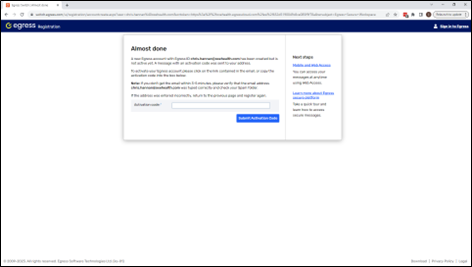
- You will receive an activation email.
- Copy the code and enter it into the browser window and click on “submit activation code”.
- In the email click on “activate account”.

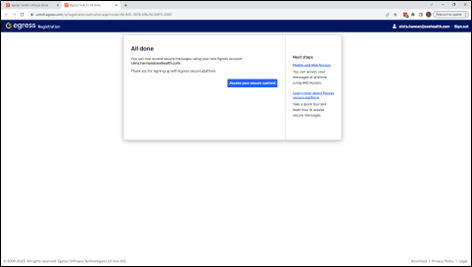
- A new window will launch in your browser that confirms your account has been set up.
- Return to the original file-share email and click the link. This will open a second browser window on the LIO Egress cloud address. Click “download” as shown below.
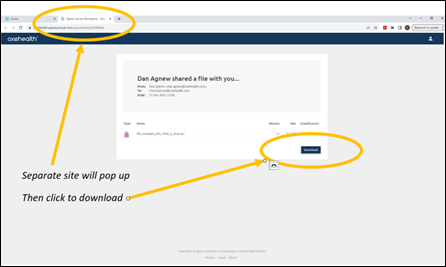
- The download will arrive into the location designated as the default download folder in your system, for example, “C:\Users\username\Downloads\” on a Windows machine. The video will remain on the Egress cloud for 29 days from the date of the email link. Responsibility for this data is now the recipient’s responsibility. LIO reminds users that the data includes personal data or private health information the handling of which may be governed by local regulations and company policies.
Document control
- Version: 1.10.
- Unique reference number: 1071.
- Approved by: clinical policy review and approvals group.
- Date approved: 15 October 2024.
- Name of originator or author: head of information quality or information quality manager.
- Name of responsible individual: chief nurse.
- Date issued: 24 June 2026.
- Review date: 31 December 2026.
Page last reviewed: July 02, 2026
Next review due: July 02, 2027
Problem with this page?
Please tell us about any problems you have found with this web page.
Report a problem